Pain in the throat can happen from many reasons. Although people may refer to the neck as the throat, what doctors consider as throat is the pharynx and the tonsillar areas. Lets have a look at the anatomy of the throat and then see how things change in disease.
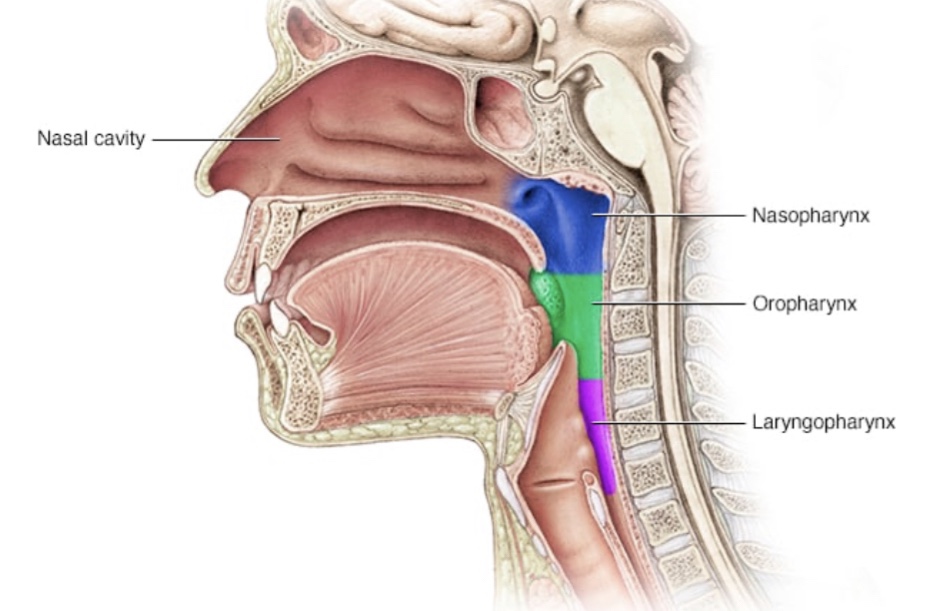
The throat or pharynx is a muscular tube that connects the mouth and the nose to the windpipe (trachea) in the front and the food pipe (Oesophagus) behind. It is divided into 3 parts, the upper Nasopharynx (the part behind the nose), the Oropharnx (the part behind the mouth) and the Laryngopharynx (the lower most part behind the larynx (the voice box).
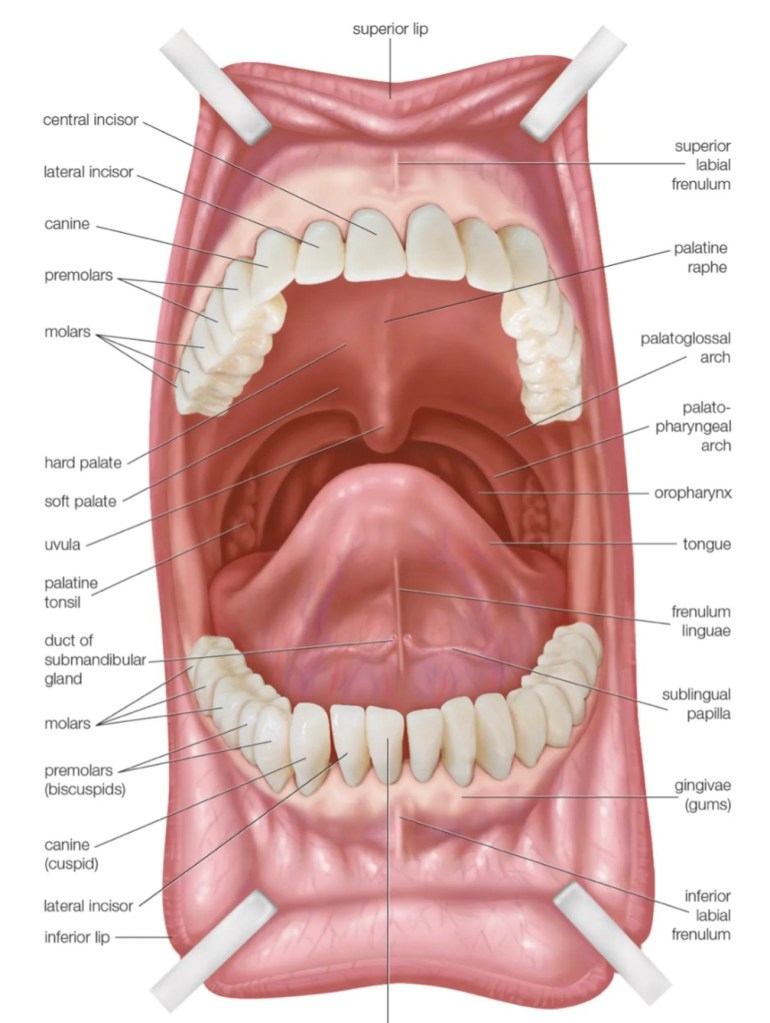
The throat or the Oropharynx is bordered by the palate on the top, the pharyngeal pillars (tonsillar areas) on the sides and the tongue below. This is the most important gateway into both the Respiratory as well as the Gastrointestinal tract and is therefore a site for frequent infections.
A sore throat occurs whenever there is inflammation in the throat. Inflammation could be due to infection or a non-infectious cause. Lets look at some of the common and not so common causes for a sore throat.
1. Viral Pharyngitis – the most common cause for a sore throat after streptococcal infection is a viral pharyngitis. This season, the commonest cause is the Covid 19 infection which causes severe and painful sore throat. Unlike a bacterial infection, the patient will have a runny nose, the throat will be erythematous (reddened) and would not show any pus points. Infectious mononucleosis (kissing disease)is seen in young patients who catch infection from kissing. The pain is often out of proportion to the severity of the pharyngitis on examination. This infection can be associated with a rash, enlarged lymph nodes in the neck and an enlarged liver and spleen. The blood smear study would show typical large lymphocytes (increased Lymphocyte count) The treatment is essentially symptomatic.

2. Bacterial (streptococcal pharyngitis and tonsillitis)
The throat shows small petichiae (bleeding spots) on the palate. If tonsillitis coexists, the tonsils are enlarged and show pus oozing from them and the lymph nodes in the neck are enlarged. Streptococcal infection is the commonest cause for a sore throat even more common than viruses. Recurrent streptococcal infection may predispose patients to Rheumatic fever and cardiac disease. Bacterial pharyngitis may also be caused by Neisseria gonorrhoea, Mycoplasma and chlamydia species. Antibiotics would be needed in many cases.


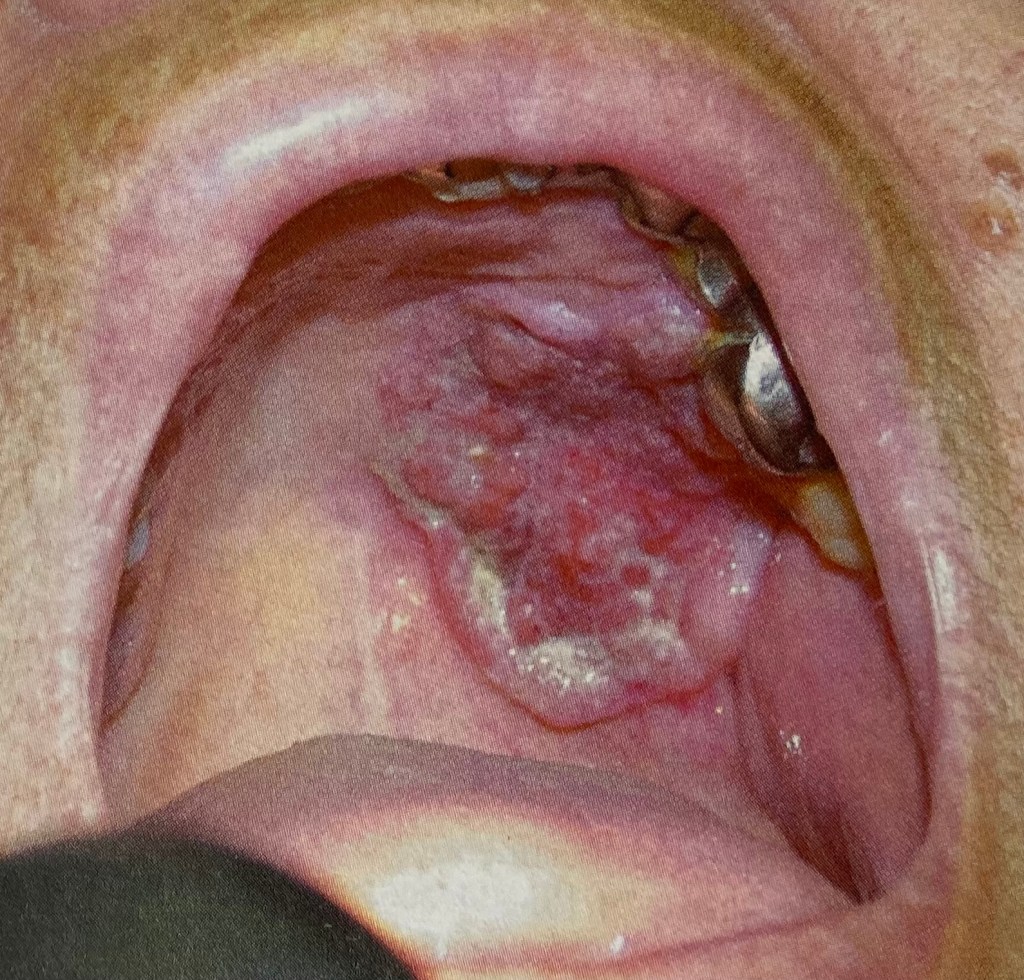
3. Peri-tonsillar abscess (Quinsy)- when the infection spreads through the capsule of the tonsil, pus collects outsides the tonsil and displaces the tonsil inwards, nearly occluding the oral cavity.Peritonsillar abscess must be treated with antibiotics and may need a drainage procedure to remove the pus and to hasten

4. Diphtheria is a respiratory tract infection that cause severe pharyngitis with a thick membrane over the throat. This can be dangerous if left untreated. Prompt antibiotic therapy will be needed.

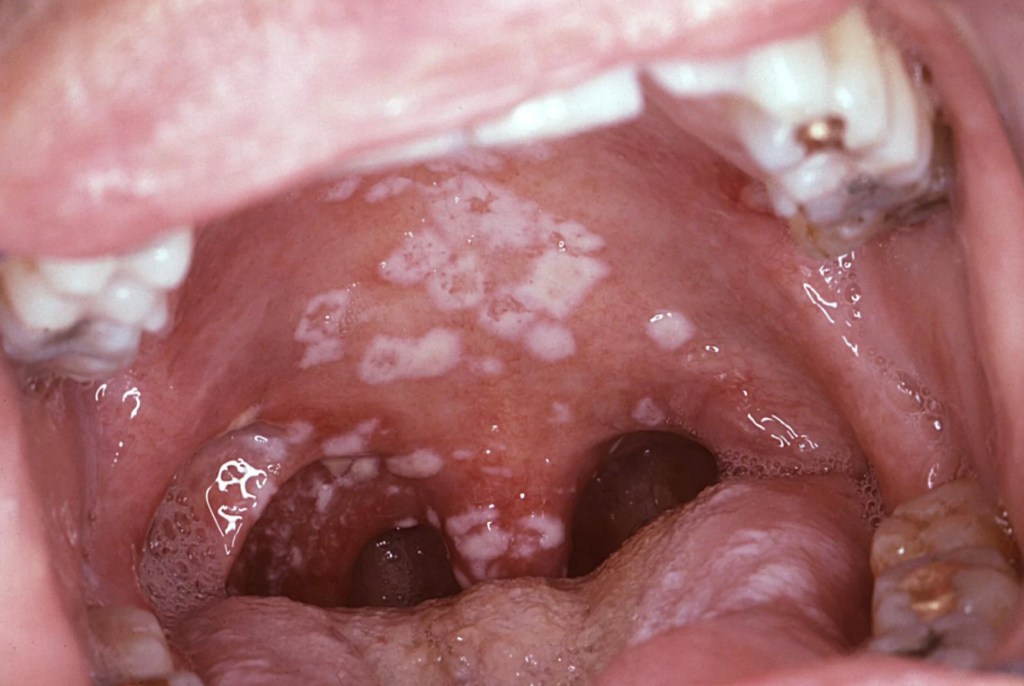
5.Oral thrush is causes by yeast like fungus called candida. This is also quite common. It is seen on those on broad spectrum antibiotics, diabetes, steroid therapy, immune compromising conditions including HIV infection. The white patches can easily be dislodged showing underlying erythema (redness) and inflammation. Anti-fungal lozenges will be very effective in its treatment along with treating the cause for the infection e.g., controlling the blood sugars and stopping the antibiotics.
Non- infective causes for a Sore throat
1. Acid Reflux with pharyngitis – this is a very common cause for chronic pharyngitis. Acid reflux is a lifestyle disease caused due to an incompetence of the gastro-oesophageal valve usually seen in obese individuals who overeat.


So if your throat is sore and you have difficulty swallowing food, please consult your doctor for advice. Once the cause for the sore throat is identified, specific treatments are given to hasten recovery. Most infective sore throats respond well to antiinflammatory medicines such as Brufen. Antibiotics will be given by your doctor as necessary. Specialist consultation may also be needed.


You must be logged in to post a comment.