Irritable Bowel Syndrome is one of the common functional bowel diseases that affect us. Intestinal diseases may be classified broadly into Organic and Functional, where Organic refers to structural intestinal disease as compared to Functional disease where an identifiable structural bowel problem like an ulcer or narrowing (stricture) or bulge (diverticula of the intestine) is absent. IBS is characterised by abdominal pain and altered bowel habits (constipation or diarrhoea).
People with IBS tend to have visceral hypersensitivity i.e., increased perception of pain on intestinal distension. Studies done on IBS patients have shown increased inflammatory/ immune cells in the intestines (on biopsy) such as lymphocytes, mast cells which secrete inflammatory cytokines, histamine, serotonin and other substances that stimulate the nerves inside the bowel wall (Myenteric plexus) and cause increased cellular permeability, pain and increased contractions of the intestinal muscle leading to diarrhoea. This could be the cause for the so called post infectious IBS that is associated with bacterial, viral, protozoal and helminthic infections. There is also a theory that composition of fecal microbiota could be associated with the development of IBS. Small intestinal bacterial overgrowth (SIBO) also has an association with IBS. Studies done have shown that people with IBS have abnormal breath tests indicating bacterial overgrowth and gets better with antibiotc treatment which can reduce the bacterial population. Food allergies, carbohydrate indigestion and gluten sensitivty are also attributed as causes for IBS. Genetic causes, psychological causes such as anxiety depression phobias and somatization have also been shown to be risk factors for IBS development.
IBS is usally suspected when symptoms of abdominal pain and altered bowel habits persist for more than 3 months. The following are typical features of IBS: The symptoms could be either intermittent or continuous.
1. Abdominal pain for atleast 1 day a week. It is usually lower abdominal.
2. Changes in stool frequency – Constipation or diarrhoea
3. Changes in stool form – lumpy hard, pellet like or tooth paste like or loose and watery!
4. Change in stool passage – urgency, need to strain or having a feeling of incomplete evacuation
5. Bloating of abdomen.
6. Association with depression, anxiety, chronic stress or somatization.
What features would suggest that IBS is UNLIKELY!
1. Alarm symptoms such as alternating constipation with diarrhoea, blood in stools, nocturnal diarrhoea, weight loss and fever might indicate a more sinister pathology such as cancer or Inflammatory Bowel disease.
2. An Acute onset might suggest an infective cause for the symptoms.
Such people with the above features and those with a family history of cancer, Inflammatory Bowel disease or Coeliac disease would need other investigations such as Colonoscopy and biopsy.
IBS is classified into 4 types. IBS with diarrhoea (bowel movement > 3 /day), IBS with constipation (bowel movement < 3/week) , IBS with both diarrhoea and constipation and IBS that is not subtyped.
A complete blood count, ESR, CRP, stool complete and occult blood test, Stool calprotectin and and a sigmoidoscopy and colonoscopy may be done (for those with alarm features only) are some of the tests that may need to be done for someone suspected to have IBS.
IBS is a chronic disorder and therefore education and reassurance go a long way in helping the patient cope with the disorder. IBS is prone to recur with periodic exacerbations and remissions. Moderate exercise is believed to be helpful. Avoidance of gas causing food may also help. A diet low in FODMAPS (fermentable oligo, di, mono sacharides and polyols may be helpful. Restriction for 2-4 weeks may improve symptoms. The FODMAPs include 6 food groups:
1. Fructose – corn syrup, apple, pear, watermelon and raisins.
2. Fructans – garlic, onions, leeks, asparagus and antichokes.
3. Wheat based foods – breads, pasta, cereals, cakes.
4. Sorbitol – stone fruits
5. Raffinose – legumes, lentils, brussel sprouts, soybean and cabbage.
Many pharmacologic agents (medicines) are being used to treat IBS.
Antispasmodics such as hyoscyamine, dicyclomine and mebeverine and Probiotics are used for abdominal pain.
Loperamide can be used for diarrhoea.
Polyethylene glycol 3350 is used for constipation predominent IBS. Newer medicines such as Lubiprostone, Linaclotide, Plecanatide and Tegaserod are also used for the same condition. Antidepressants such as Tricyclics and SSRI are also useful. Rifaxamin, a non-absorbable antibiotic is used with good effect for bloating.
Cognitive behaviour therapy, yoga, relaxation and hypnotherapy is also believed to be helpful.
Fatigue is not an uncommon complaint that a doctor hears at his clinic. This term however could mean many things to many people. While there are many normal causes for fatigue and tiredness, I would like to write about the abnormal (pathological, disease related) causes for tiredness that the reader needs to be aware of.
Fatigue could happen normally from doing unaccustomed severe exertion or exercise or due to inadequate rest and recovery after exertion, sleep deprivation, travel thorough different time zones (Jet lag) or due to obesity, under nutrition and severe emotional stress. You could recover from fatigue from the above causes by taking adequate rest. So why should fatigue persist even after taking enough rest and what could the reasons be for it?
Pathological fatigue has many causes. Broadly they may be grouped into the following categories.
Significant Fatigue is when fatigue persists for at least 2 weeks and can affect upto 25% of the population at some time. Chronic sleep deprivation (sleep apnoea) can also be a cause for severe fatigue.
Chronic Fatigue is when fatigue affects the person for more than 6 months.
Alarm signs in Chronic fatigue:
1. Anorexia and weight loss (>10% per 6 months)
2. Enlarged Lymph nodes.
3. Memory and concentration impairment
4. Inability to function due to myalgias, arthralgias, headaches etc.
5. Deep depression
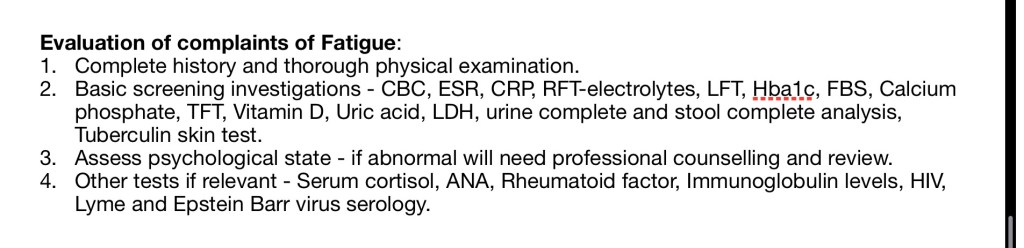
Evaluation of complaints of Fatigue:
Treatment of Fatigue
Identification and treatment of the cause for fatigue will cure the problem most of the times`.
Interventions that may be of benefit for people with problematic fatigue are:
1. To fix lifestyle abnormalities – to regulate lifestyle, to eat, sleep on time.To exercise regularly – resistance as well as aerobic training reduce fatigue. (Graded exercise programme)
2. Use of nocturnal cPAP for those with Obstructive Sleep Apnoea
3. Medications – Melatonin or nocturnal sedatives
– Modafinil or Armodafinil
– Testosterone replacement therapy for those with deficiency
– Steroid replacement therapy for those with adrenaline insufficiency
– Correction of Vit D and other vitamin deficiencies.
4. Cognitive Behaviour therapy provided by an experienced psychologist.
A note of Long Covid Syndrome:
Covid 19 infection has been the most common cause for prolonged fatigue over the past 2 years. Long covid syndrome refers to the persistence of symptoms many weeks after the acute infection. Fatigue is a persisting symptom irrespective of the severity of the infection. In one study 92% of covid patients had fatigue 79 days after the onset of Covid infection.
Common symptoms of long covid include:
Fatigue,breathlessness, chest pain,mental fudge and cognitive abnormalities, sleeplessness, smell and taste abnormalities, headache and feverishness etc. Treatment is essentially symptomatic only.
I am currently reading a book called The Anarchy by William Dalrymple, a book detailing a state of anarchy existing in India in the eighteenth century which made it easy for the British East India company to defeat the ruling Kings and take over the country. Apparently at the time when Lord Cornwallis ran the EIC, Britain had lost its American colonies to the descendants of the original european settlers (and not the locals). In India, one in three British men were “cohabiting” with Indian women and it was believed that there were 11000 Anglo-Indians living in the 3 Presidency towns ( Madras, Calcutta and Bombay). Fearful of losing their Indian territories in the future to the descendants of British men, the EIC banned all Anglo-Indians “orphans” from serving in the company army (as well as in the civil and marine branches of the EIC) and from owning land thereby excluding them from most lucrative sources of employment. They were only allowed to work as pipers, drummers and farriers in the company army and were further demoted to holding minor jobs as clerks, postmen and train drivers. The Anglo- Indian community was therefore relegated to the fringes of Indian society where they developed their own unique culture and spoke English in their own unique style. My father had told me many years ago that “bloody” and “bugger” were words used primarily by the Anglo-Indian communtiy and that it subsequently become common usage. I remember using these words without knowing their meaning as a child, at home in front of my parents and never being corrected or admonished. So kindly excuse my use of those words in this article.
So, this article is written to give you more information of the common causes for anaemia, why they happen and give you some information as to what you can do about it. I write this article from my perspective and experience as a doctor practising in an urban setting in South India.
Low hemoglobin in referred to as Anaemia. Men are anaemic if their hemoglobin in less than 13.6 gm/dl (hematocrit <41%) and in women if hemoglobin is less than 12gm/dl (hematocrit <36%). Worldover, the commonest cause for anemia is Iron deficiency.
Hemoglobin serves the very important function of carrying Oxygen to all the tissues. Oxygen is picked up in the lungs and delivered to the tissues in every corner of the body. Therefore when anemic, the person may feel breathless on exertion (or even at rest when severe), tired, dizzy with chest pain, cold extremities and pallor. The person could also be absolutely asymptomatic especially if the anemia develops gradually over several months or years.
The cause of the anemia could vary according to the age at detection. In children, Nutritional Iron, B12 and folate deficiency, Hook worm infestation, Hemolysis and heriditary causes (Thalassemia or Sickle cell anemia) may occur.
In adults, Iron deficiency due to Acute or chronic blood loss (menstrual blood loss, Gastrointestinal bleeding from piles, stomach ulcers etc worsened by antiplatelet drugs such as Aspirin or Clopidogrel), Kidney failure, chronic diseases and Cancer chemotherapy.
In the elderly, anemia can be caused by Chronic diseases, Iron deficiency (from gastrointestinal blood loss), Vit B12/Folate deficiency, Chronic leukaemia and cancers, Myelodysplastic disorders and blood loss (acute from fractures after falls and chronic from intestinal bleeding).
Broadly Anaemia can be divided into the following categories:
Reduced production of blood
Deficiency Anaemia – Iron, B12 and Folate.
Bone marrow disease – Acute and Chronic leukaemia, lymphomas and other bone marrow malignancies, Aplastic anaemia, Myelodysplastic syndrome, Myelofibrosis and Infections affecting the bone marrow.
All blood cells are produced in the bone marrow and any disease that affects the bone marrow can cause anaemia.
Anaemia of Chronic disease – Chronic disease such as Inflammatory bowel disease, Rheumatoid arthritis affect the transfer of iron from the immune cells to the bone marrow.
Anaemia of Kidney failure – the kidneys produce Erythropoietin, a hormone that stimulates the bone marrow to produce blood. When this stimulus reduces due to kidney failure,anaemia ensues.
Increased Blood destruction or loss
Blood loss – acute and chronic.
Hemolytic – Heriditary (Hemoglobinopathies), Autoimmune, Enzyme defects(G6PD), MAHA
Malaria
Overactive spleen (Hypersplenism)
So how do you go about finding out the cause for your anaemia?
The following tests would be useful.
The CBC – complete blood count
Hemoglobin levels – based on the hemoglobin levels anaemia can be classifed as mild (>10gm/dl) moderate (7-10gm/dl) and severe ( <7gm/dl).
MCV – mean corpuscular volume
– A low MCV occurs frequently in Iron deficiency and a high value >100 in Vit B12 and folate deficiency.
Platelet counts – are reduced in acute infections and Vit B12 and folate deficiency and Bone marrow disease. A high platelet count is seen in Acute as well as chronic blood loss.
ESR – increases in all Anaemias.
CRP – increases in all inflammatory and infective conditions.
Reticulocyte count and index – A normal or increased Reticulocyte count and index indicates a functioning bone marrow and could indicate blood loss or hemolysis as a cause for the anaemia.
Peripheral smear – especially reported by a human rather than an automated machine will give a very valuable information regarding the cause for anaemia.
Iron study – Serum Iron, Transferrin saturation and Ferritin – Low serum iron, low transferrin saturation (low TIBC) and a low Ferritin indicate iron deficiency. A normal or high iron, normal or low saturation and a high Ferritin level would indicate Chronic infection and inflammation.
Serum LDH – lactate dehydrogenase – rises in hemolytic anaemias and other hematoloic conditions.
Stool for occult blood – positive report would indicate gastrointestinal blood loss.
Serum Vit B12 and folate levels – are reduced in Megaloblastic (macrocytic) anaemia due to B12 and folate deficiencies.
Renal function test – Urea and creatinine – Creatinine levels > 4 mg/dl may indicate a renal cause for Anaemia.
Other tests:
Haemoglobin electrophoresis – can help diagnose Thalassaemias.
Bone marrow aspiration and biopsy study – Will indicate if an underactive bone marrow is the cause for the anaemia.
Osmotic fragility – Increases in Heriditary spherocytosis.
Coombs test – is positive in Autoimmune Hemolytic anaemias.
Normal blood smear showing RBC with central pallor (1/3 diameter of the cell). The large purple cells are the white cells and the small ones (11’o clock position) are the platelets.The smear above shows iron deficiency anemia, the central hollow is more than a 1/3rd of the whole red cell. The red cells are of smaller sizes and different shapes.The smear above show megalobalstic (macrocytic) anemia with large red cells and hypersegmented Neutrophils in the lower centredue to Vit B12 or Folate deficiency.
Case studies: Lets have a look at a few case stories from my practice.
1. Mrs. M was a 38 yr old lady who was seen by her gynaecologist for anemia and was prescribed iron tablets as emperic treatment of Iron deficiency anemia due to menstrual blood loss.I had seen her a month later for severe abdominal pain and constipation.As her stool occult blood test returned positive, a colonscopy was done and it showed a large growth nearly occluding the rectal lumen (and she had been absolutely asymptomatic till then).She underwent surgery to relieve obstruction and later succumbed to the cancer despite best therapy.
Moral of the story- every case of suspected anaemia needs relevant investigations!
2. Mr. A was a 21 yr old man studying in Canada. He was my patient since the age of 16yr and his parents were always unhappy that he was a poor eater and liked only junk food like pizzas and bread! He was brought to my clinic by his father who was concerned that his son looked weak, the blood tests done revealed anemia which was thought to be due to iron deficiency as it was of the microcytic type.I ran a set of tests on him which showed that his iron levels were normal. A Hemoglobin electrophoresis test done revealed Thalassaemia minor. In this case giving iron tablets would have been the wrong thing to do.
Moral of the story- every case of anemia needs relevant investigations!
3. Mr.S was a 36 yr old patient of chronic deforming Rheumatoid arthritis. He gave a history of previous blood transfusions for anaemia and of regular intake of pain killing tablets for his joint pains. His Hemoglobin was 3.5gm/dl, ESR and CRP were very elevated, the iron study revealed low iron and elevated ferritin levels and the stool occult blood test was negative. He was diagnosed to have anemia of chronic disease. He was transfused to hemoglobin of 8gm and was started on DMARDS for his Rheumatoid arthritis.
Moral of the story – not every case of anemia is due to Iron deficiency.
4. Mr. H was a reformed alcoholic who came with complaints of weakness and tiredness. His examination revealed signs of chronic alcoholic liver disease with ascites (abdominal swelling due to fluid collection). Investigations revealed moderate anemia with hemoglobin of 8gm/dl, pancytopaenia (reduction of Red cells i.e., anaemia, white cells and platelets) and fecal occult blood test was positive. He was diagnosed to have anemia due to hypersplenism and due to GI blood loss. The patient was transfused to a hemoglobin of 10gm/dl, his coagulation disorder was corrected and he had a endoscopic procedure to treat his bleeding varices.
Moral of the story – your doctor can find clues to the cause of anemia. So if you are anemic, go see your doctor and get it corrected.
5. Mr. N came to see me with some dyspeptic symptoms. His hemoglobin was 8gm/dl and his MCV was 105. His peripheral smear showed macrocytic anaemia suggestive of megaloblastic anemia with hypersegmented nuclei on Neutrophils. He tested postive for anti Intrinsic factor antibodies, his vit B12 levels were very low and an endoscopy done revealed atrophic gastritis. He was diagnosed to have Pernicious anemia due to Vit B12 deficiency and was given IM injections of Vit B12 after which his hemoglobin returned to normal.
Take home message: If you are anaemic, get some tests done, see your doctor before you start giving any excuses to explain why you are anemic.
Sleep is a recurring natural state of mind and body characterised by reduced consciousness, reduced sensory activity and perception, reduced muscle activity (increased muscle relaxation) and consequently reduced interactions with the surroundings.
Sleep is essential for all animals and is when the body builds up, restores energy and every other system (muscular, nervous, endocrine and immune systems) during this period of rest. Inadequate quantity and quality of sleep can lead to a variety of diseases including diabetes, heart disease, strokes, obesity and depression and other psychiatric disorders.
Modern living with long working hours, working through the night, travelling through various time zones, use of various electronic gadgets (Blue light emitted by mobile phones tablets and laptops supposedly inhibit the release of the sleep hormone melatonin) disrupt normal sleep and lead to typical stress related disorders.
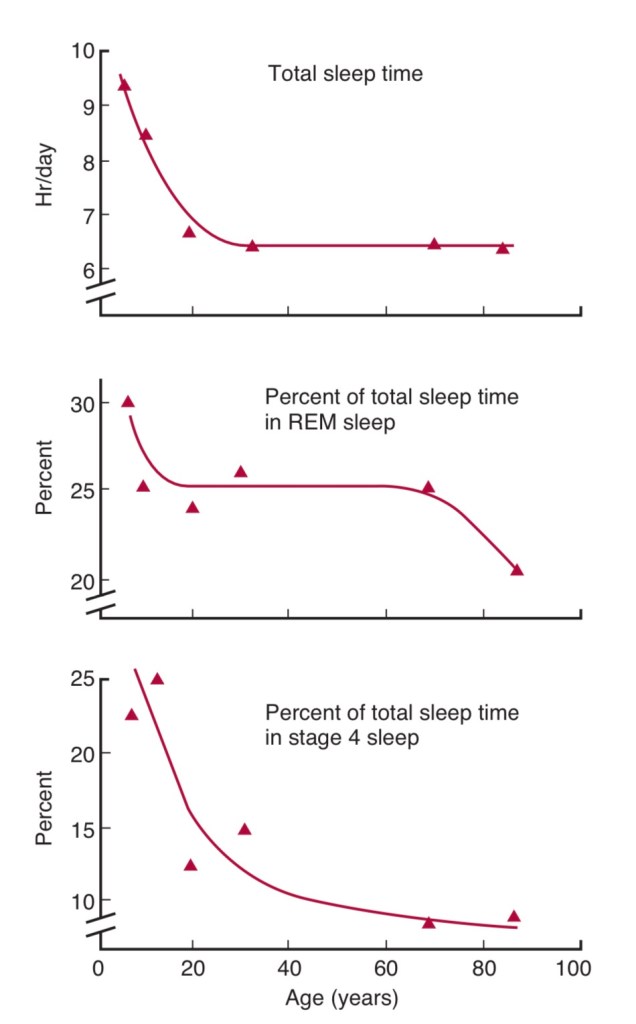
While each person requires different amounts of sleep, on an average a 40 yr old needs 7 hr every night, 6 1/2 hrs of sleep at ages 45-60 and about 6 hrs or less at the age of 80 yrs and above.
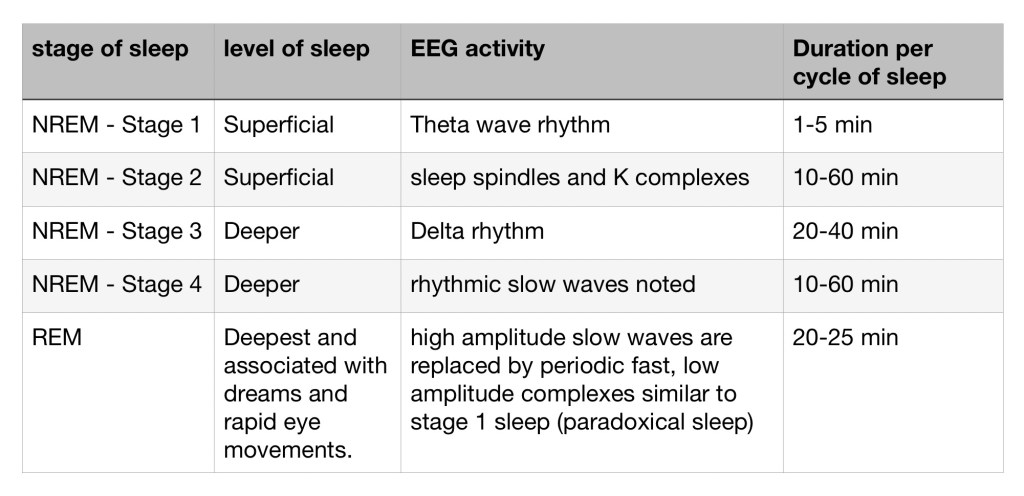
Sleep occurs in cycles that last 90-110mins (i.e., less than 2 hr). Each cycle has 2 types of sleep, NREM (non rapid eye movement or slow wave sleep) and REM (Rapid eye movement sleep). NREM has 4 stages 1,2,3 &4). When we close our eyes to sleep , we are in stage 1 and we gradually move into the other stages as we continue to sleep. Stages 1 and 2 are the lighter planes of sleep and 3 and 4 are the deeper planes. Throughout each stage the body relaxes progressively and the EEG (brain activity) changes and slows down.
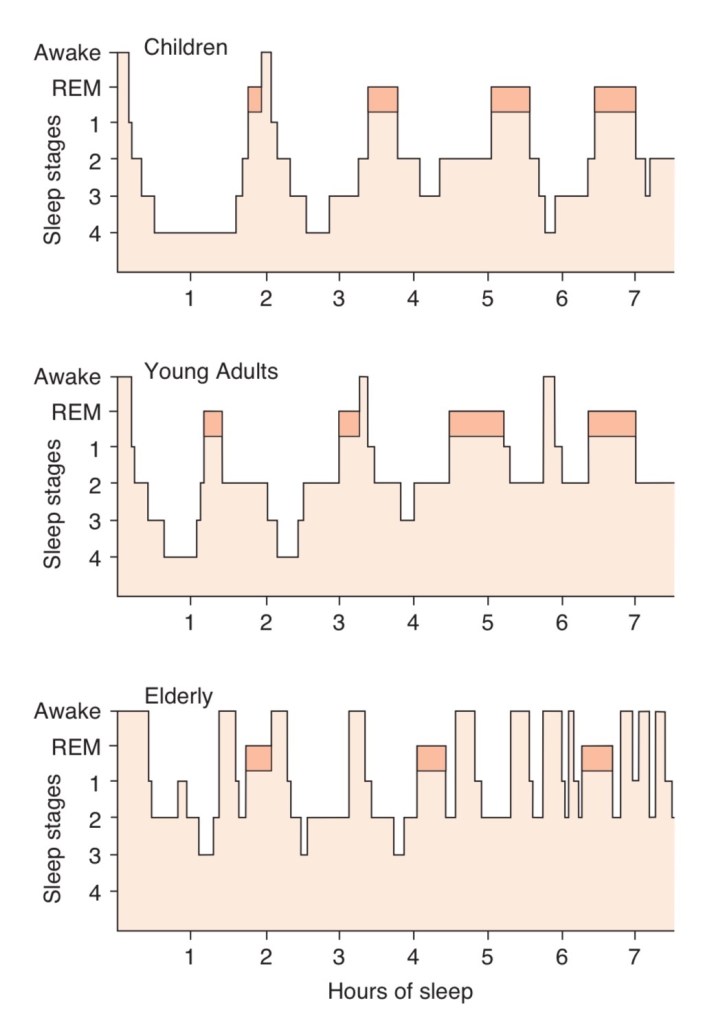
REM sleep deprivation leads to sleep that is not restful. More time is spent in stage 3-4 during the first half of the sleep period. In the second half, more REM sleep happens as shown in the diagram. As REM sleep is most restful, staying awake during this period (between midnight to 4AM) has health consequences. Younger children especially newborns spend much longer times in stage 4 sleep and REM sleep. REM sleep duration reduces with ageing to much less than the 25% enjoyed by young adults.
You may have a sleep disorder if you have trouble falling asleep when you lie down in bed, if you wake up feeling tired and if you tend to doze off during the day especially during work.I had a friend who fell asleep at the wheels of his car and had a serious accident. If these are issues for you, the question may arise if you should buy a smart device to track your sleep. Unfortunately most of these devices that are worn on the wrist are not medically validated to diagnose sleep disorders. Most of them detect body movements or in some cases the heart rate and its variability, to decide if you are asleep or awake. These devices could get fooled into believing that some insomniacs are asleep when they have their eyes closed, body relaxed and are in bed waiting to fall asleep. So while these devices may be accurate in detecting duration of sleep (based on movements etc), they can be quite inaccurate when they calculate the time spent in the different stages of sleep and also when they make assumptions about the quality of sleep. My smart device suggested that I had sleep apnoe when it detected that I woke up 20-25 times during the night. As I didnt have any symptoms of a sleep disorder, I concluded that it probably detected my movements in bed and inferred that I had woken up. The sleep specialist whom I discussed this also came to the same conclusion. On the other hand, validated sleep study devices (Polysomnography) monitor various parametes such as EEG, ECG, Muscle tone, chest and abdominal movememts, O2 saturation and limb movements to give a detailed analysis of sleep. Compared to these devices, sleep trackers are only 78% accurate in detecting sleep vs wakefulness, 38% accurate in identifying exactly how long it took to fall asleep and only about 50% accurate in detecting the various stages of sleep (including REM sleep).
So should you by a sleep tracker? I believe that anything that is measured, improves. Therefore if you aren’t sleeping well, it may be a good idea to buy a sleep tracker. Many of these devices also measure your heart rate during sleep and an increasing RHR (resting heart rate) may also be indicative on a non-restful sleep.
I have used the Samsung Galaxy watch 3 which is excellent for sleep monitoring and the apple watch which is more accurate for heart rate monitoring (especially during exercise). So go ahead and buy a smart watch that can track your sleep, focus on all the things that you need to do to stay healthy and get healthier!







You must be logged in to post a comment.