Alopecia or hair loss can be divided into 2 main categories.
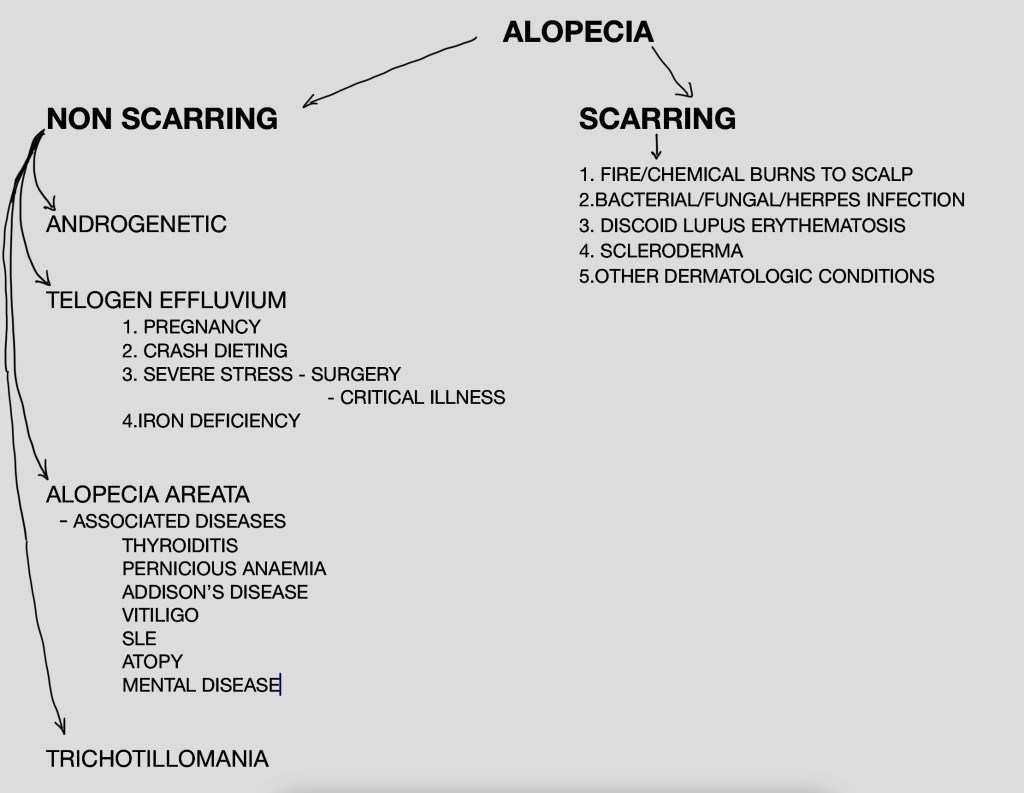
Non-scarrring alopecia is diagnosed when there is obvious hairloss and on close examination of the scalp, hair follicles are clearly visible. This form of alopecia is often reversible.
Scarring Alopecia occurs when the full thickness of the scalp is damaged from a variety of causes leading to scarring and typically scars lose their hair follicles and the skin appears smooth. Scarring alopecia is permanent and nothing can reverse the damage done.

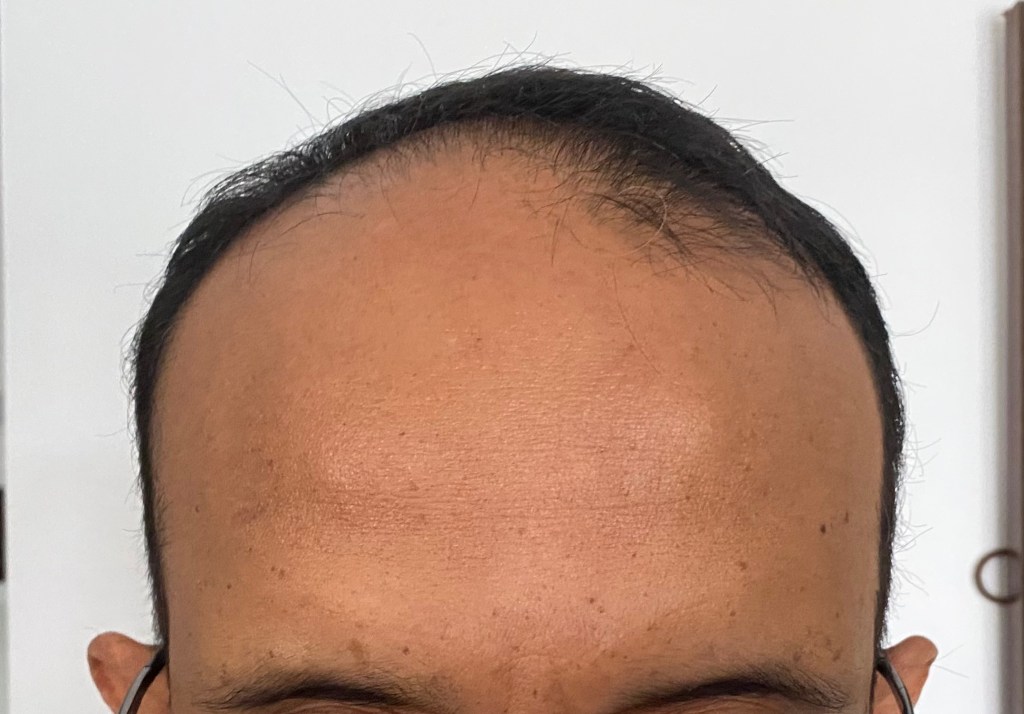
Androgenetic alopecia occurs in both men and women. Typically the hairline may receded (at the temples) and hair loss may become obvious either as thinning of hair “on the top” or as balding of the crown (top of the head).

Telogen effuvium refers to resting hair. Severe stress (to the body) from any cause leads to cessation of growth of the hair follicles and therefore hair becomes weak and falls. Apart the causes already mentioned in the box above oral contraceptive use, cancer, high fevers due to infections can cause this kind of hairfall.
Alopecia areata is a kind of alopecia that is believed to be due to a unknown autoimmune disease process. Typically the hair is broken near the skin giving rise to the typical exclamation mark hairs. Clearly circumscribed areas of hairfall are noted on the scalp. Alopecia areata totalis is when there is complete hair loss from the head including the eyebrows and lashes.

Trichotillomania refers to predominently unilateral (on the side of the dominant hand) hairfall due to habitual,probably absent minded pulling on the hair.
Traction alopecia is often see in girls who tie their hair tight.

Other scalp conditions such as fungal infections, dandruff etc can also cause significant hairloss.
Investigations that may be useful in people with hairfall include:
Routine screening tests: CBC, ESR, LFT, RFT-E, Lipid, Urine complete.
Specific tests: Serum Iron, Transferrin saturation, Ferritin, serum Testosterone, DHEAS,TFT,Vit D, Vit B12, Folate.
Other tests that may be done on doctors discretion: Thyroid antibodies, ANA, Fasting cortisol assays and scalp (skin) biopsy.
Usual treatment that is offered to patients who have hairfall!
Minoxidil 5% hair lotion to be applied twice daily and Tab.Finasteride 1% (for men) and upto 2.5% fo women for upto a year can lead to dense hair growth and can be tried for all forms of nonscarring alopecia.
Intralesional steroids or oral steroids is given to patient with alopecia areata. Oral JAK inhibitors like Tofacitinib and Ruxolitinib are also being used for AA.
Counselling and prescription of N-Acetyl cysteine 1200-2400mg orally every day for 3 months can be effective for Trichotillomania.
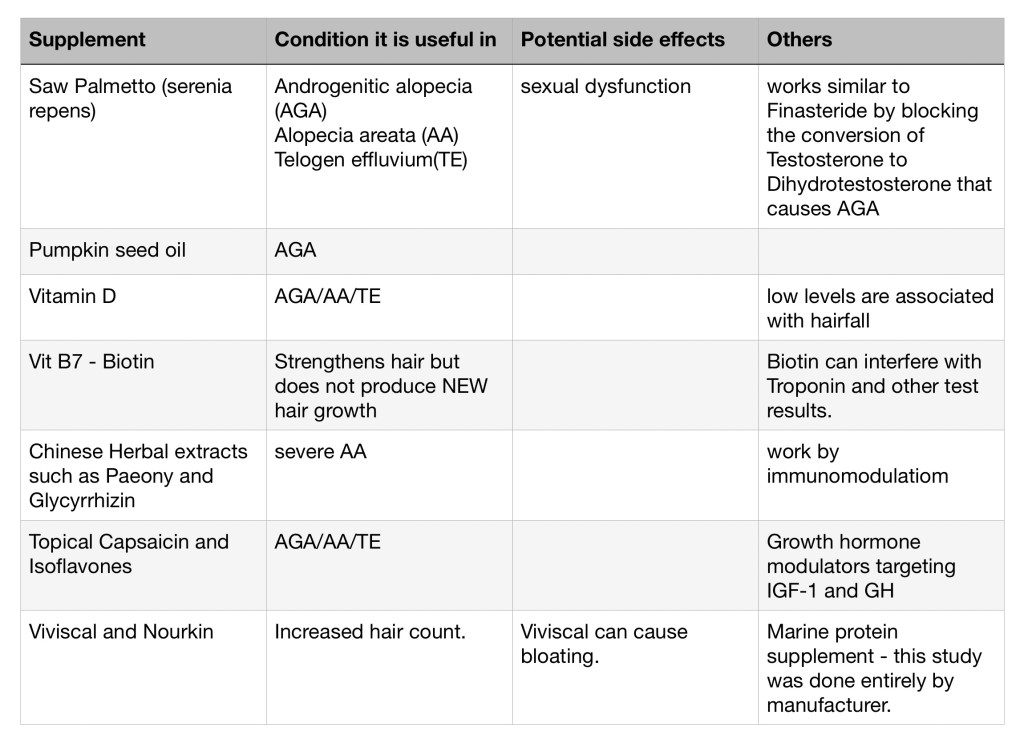
What supplements may be beneficial for hair fall?
Very many people take supplements for hairfall. I came across a recent article where the authors had screened 6000 odd citations and selected 20 articles with relevant information about use of supplements for hair fall. Here are the excerpts from the article.
Things to do before starting yourself on supplements for hairfall/loss are: Consult your doctor and discuss the pros and cons of supplementation, get some blood tests to identify deficiencies of vitamins, minerals and other nutrients accept that supplements may not have predictable effects and that they may also have some side effects.





You must be logged in to post a comment.