Just today, I lost possession of my phone for a short while. I was quite upset, in fact so upset that I developed some gastritis with severe pain in my tummy. And also today in the case folder of one of my patients, I saw a small scribble on stress that I had made in his case file to help him cope with the situation in his life. So I thought it would be the right time for me to rethink my response to my stress and see how I can deal witth them in a better way in the future and to put down my thoughts on paper. I hope you enjoy reading this article and get something useful out of it.
Stress is usually not something someone does to you but is actually something that you do to yourself when faced with an unpleasant situation or a person or have to make a tough decision. We need to make decisions in every situation in our lives. To stand or to sit, to talk or to stay quiet, to run or to fight. Quite often, we are stuck and find ourselves paralysed and indecisive because we think too much of the consequences of our impending decisions and actions. For example today when my phone went missing, initially I was extremely worried because the phone contained all my passwords and I was worried of the consequences of what would happen if it got into the wrong hands. It took me a while to realise that the missing phone was an iPhone with a complicated password that very few people knew and also that I would be able to lock it remotely if I lost it forever. However the phone had just fallen out of my pocket near my clinic and it was returned to me by those who found it.
Let’s look at the stress diagram below. It is said that a picture can say a 1000 words!
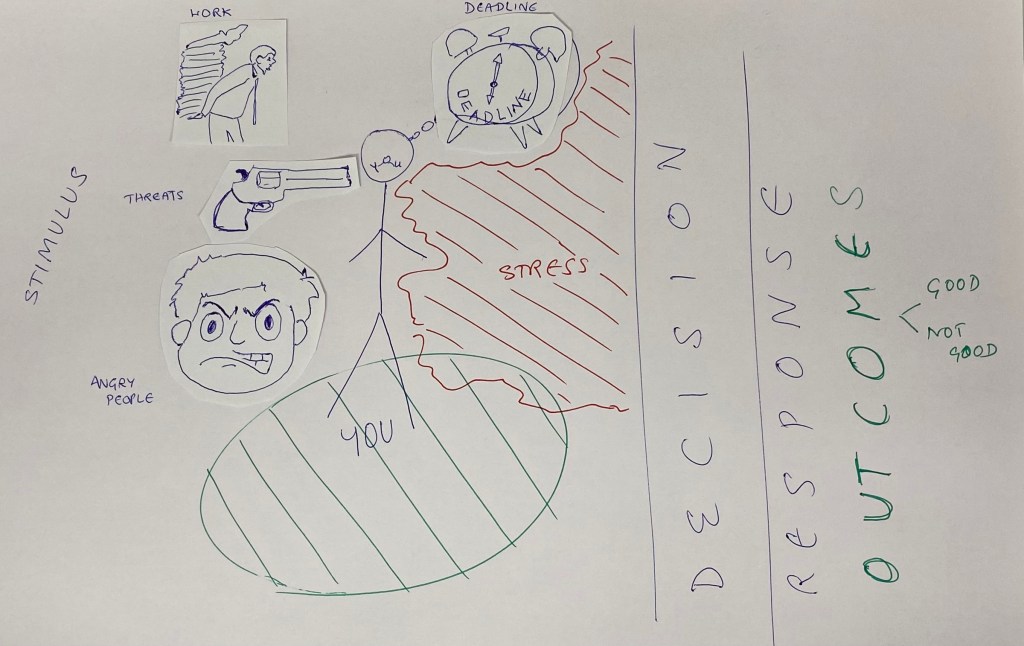
Stress is what happens to you when you are faced with a difficult situation. Stress is what happens to you before you make your mind up, before you make your decision to take action! Every stimulus demands an action. And in this gap lies STRESS! Most of us think about what happens after our actions and worry if the decision and subsequent actions are the best options to take and of how it would affect us! So fear sets in before the decision is made, adrenaline is secreted in the body, the heart starts to race, the BP shoot skywards and a whole set of stress hormones are released causing palpitations, headaches, sweating, tiredness and more. Once the decision is taken, the pressure is off and things slowly return to normal. When this happens repeatedly, it damages the body from within causing various diseases. (hypertension, diabetes, heart attacks, strokes etc).
I could make a few recommedations to you on how to handle stress.
1. The first way would be to take your own time to respond to a particular stressor. Most often we are under pressure to react immediately. e.g., if someone hits the car you are driving from behind, most of us would react by flying into a rage, confronting the offender, abusing him and sometimes even throwing punches. What if you could keep your cool, empathise with the other person and DECIDE not to lose your temper no matter what! If you could handle this situation without losing your temper you could reduce stress considerably. You could decide to give 10 min before your reaction.
2. Having a positive and happy outlook to life will also reduce your stress levels significantly. I have a friend who constantly broods that the world (or the system that is currently running our world) is coming to an end and that there will be anarchy and mayhem. Such a negative worldview would definitely handicap your handling the difficult situations in your life. How bad can life be if you imangined that the whole world is conspiring against you and people are out to get you!
3. Dont worry about consequences when you are choosing your decisions and actions. Decision paralysis leads to stress. Decisions can be changed and your course can be corrected at a later time. Nothing is final and nothing would cause irremediable harm to anyone. Staying in motion reduces stress so make your decisions and take your actions, correct course if you dont like the results of your decision but move on! Dont Stop!
4. You can only change yourself! You cant change anyone else in this world. A story has been told about a man who tried to change the world in his youth. In his middle age, he decided that the world could not be corrected and so decided to change his children. In his old age , he realised that he couldnt change his children and so attempted to change his loving wife of 50 yrs (unsuccessfully). Only on his deathbed did he realise that his life would have been very much easier if he had changed himself instead of trying to change others. So dont expect the world to change for you and you can change if you dont allow your ego to stop you.
5. Ask for help. You will be surprised how many will turn out to help you when you ask them to! The world is full of good people wanting to help their friends. Having helpful friends will reduce stress.
6. Always be on solution mode. Thinking of problems all the time leads to stress. Find solutions to problems, take decisions and don’t expect your decisions to be perfect. If you are wrong, apologize unreservedly and move on. Ask for help unashamedly. You only live once, why stress about anything. After you have made your best choice/ decision, accept whatever follows and keep moving.
7. Exercise daily and exercise well. A fit body can handle all the stress that life throws at it.















You must be logged in to post a comment.