1 in 2 women and 1 in 5 men above age of 50 suffer a osteoporosis related fracture in their lifetime. Bone mineral density is a balance between osteoclastic resorption and osteoblastic formation. Numerous hormonal and dietary factors influence the balance between bone production and resorption. However Osteoclasts work faster than osteoblasts leading to bone loss after menopause. Osteoporosis is typically asymptomatic until a fracture occurs, spine and hip fractures are the most common.
What are the risk factors for osteoporosis?
Advancing age (>70 yr), previous fragility fractures, steroid therapy, parental history of hip fractures, low body weight (BMI <20-25), current cigarette use, excessive alcohol consumption physical inactivity are risk factors for osteoporosis.
What are the medical conditions that are associated with osteoporosis?
Endocrine conditions such as hyperthyroidism, hyperparathyroidism, Diabetes mellitus, steroid excess, hypogonadism (primary or secondary to Androgen deprivation therapy), Systemic conditions such as malabsorption (Inflammatory bowel disease, Primary biliary cirrhosis and after gastric bypass surgery), malignancies (myeloma and mastocytosis), Chronic kidney failure, chronic lung disease (COPD), Rheumatogic conditions and drugs such as anticonvulsants, steroids, aromatase inhibitors, cancer chemotherapy, heparin, lithium and hormonal (antihormonal) therapies and infections such as HIV are associated with Osteoporosis.
How is Osteoporosis diagnosed?
Osteoporosis is diagnosed based on the DEXA scan and using an online tool called the FRAX score.
Who should be screened for osteoporosis?
Women older than 65yr and men above 70yrs should be screened. If the age is between 50-69, they can be screened if they have risk factors or if they suffer from conditions mentioned above that cause osteoporosis.
How is the DEXA scan interpreted?
The DEXA scan gives two values, the T score and the Z score (which is the score matched to age and gender). The Z score is used when the DEXA is done for men <50 yrs of age, healthy premenopausal women and children. (Z score of -1 to -2.5 indicate Osteopenia and > -2.5 indicate osteoporosis)
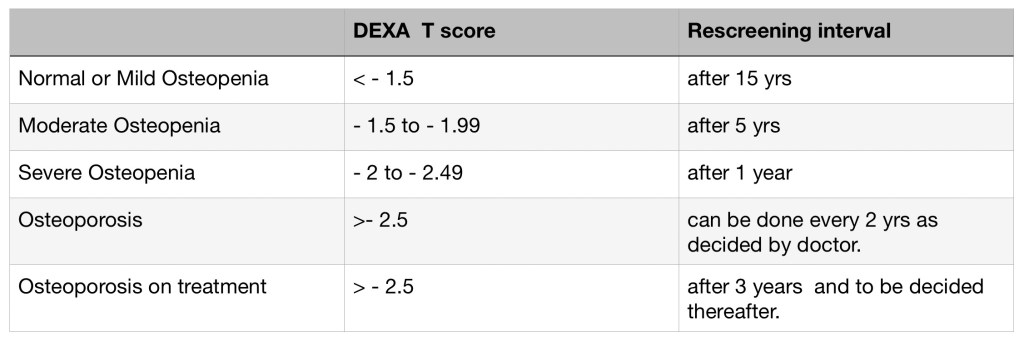
How frequently should the DEXA scan be done?
The recommedatons for the frequency of the DEXA scan is based the result.
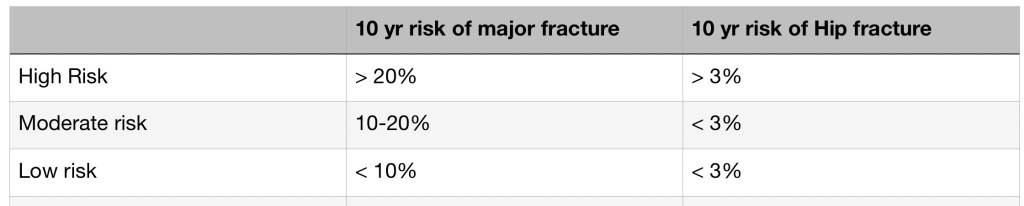
How do you interpret the FRAX score?
The T score from the DEXA scan can be misleading as it has been validated only on white women and may not be accurate for others. The WHO therefore developed the FRAX score which gives an estimate of the 10 yr risk of an osteoporotic fracture and could help planning appropriate treatment for the condition.
How is Osteoporosis treated?
1. To correct lifestyle risk factors: patients must be encouraged to eat healthy, stop cigarette smoking and take alcohol in moderation, to exercise regularly (antigravity exercises) and weight loss. A fall assessment must be made and all possible interventions to prevent falls must be made.
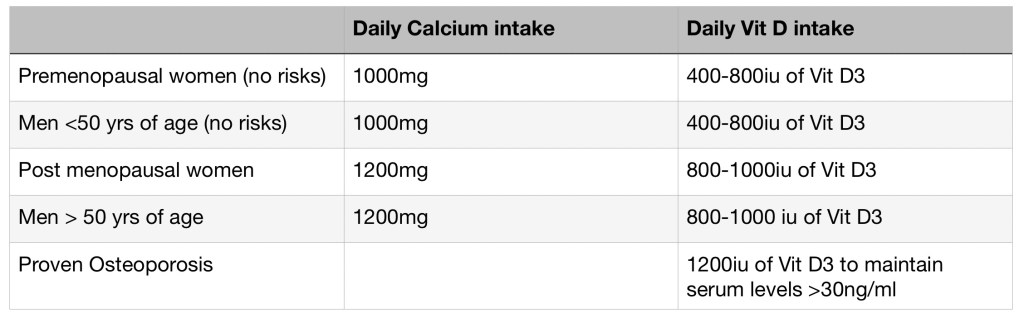
2. Calcium and Vit D supplementation: as below
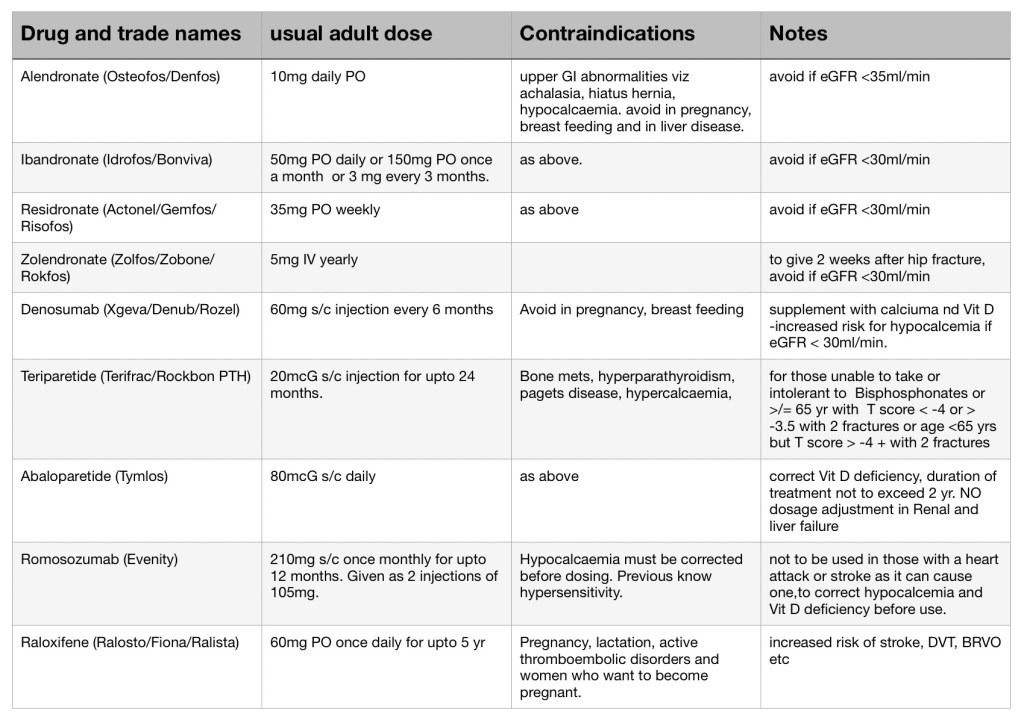
3. Medical management of Osteoporosis?
Initial management would include resorption inhibitors call bisphosphonates. Oral medications include Alandonate, Residronate and Ibandronate. Annual intravenous medications are also available such as Zolendronate. Those intolerant to Bisphosphanates or unresponsive or have contraindications can be started on Denosumab which is a monoclonal antibody directed towards the osteoclast and therefore reduces bone resorption. Denosumab course must be followed by bisphosphonate therapy. Bisphosphonate therapy isnt forever. Oral bisphosphonates must be stopped after 5 yrs and i.v Zolendronate must be stopped after 3 yrs of use (3 annual doses).
If antiresorptive therapy doesnt help anabolic agents such as Teraparatide, Abaloparatide or Romosozumab and Estrogen antagonist such as Raloxifene can be tried. Teriparetide must be stopped after 12-26 months of continuous use and must be followed up with Bisphosphonate therapy.

You must be logged in to post a comment.