Gynaecomastia is quite a frequently encountered condition in medical practice and it refers to the presence of a palpable enlargement of the male breast. Overall the incidence of gynacomastia is increasing throughout the world across a variety of age groups for a various reasons. Some of the causes attributed are endocrine disrupting chemicals in an increasingly polluted world, obesity, anabolic steroid (androgen) abuse, widespread use of medications that cause gynaecomastia and increased prevalence of diseases that cause gynaecomastia such as testicular cancer.
Gynaecomastia is common amongst teenage boys and also in elderly people who gain weight rapidly. Gynaecomastia can occur in upto 60% of pubertal boys (usually tall or obese teenagers) under the influence of hormones and most would spontaneously subside within a year.
What are the common causes for Gynaecomastia?
Often gyanecomastia occurs when an adult puts on weight very quickly. Even in pubertal children the incidence peaks between the ages of 12-14 in response to increased and fluctuating levels of male and female hormones that are secreted by the body. Most often (70% of the times) breast size would regress within a year. So when should one seek medical help and intervention?
In a teenage boy, persistence of breast tissue above the age of 17 or a sudden increase in size with pain may necessitate a visit to the doctor’s clinic. In adults, asymmetric breast enlargement especially if located below the areola of unusal firmness/hardness with nipple changes (retraction, eczema or bleeding) should alarm the individual enough to see a doctor.
The doctor after doing a thorough examination might ask for a few tests. Screening tests may include blood tests like Liver function and kidney function tests,hormonal assays of LH, FSH, Prolactin, Free and total Testosterone, Estradiol, beta hCG and thyroid function. Other scans such as Ultrasound breast, testes, CT for chest and adrenal glands and a FNAC may also be suggested.
Treatment is usually indicated for painful large breast masses (>5cm) in size with worrying features such as nipple bleeding or discharge, eczema or enlarged lymph nodes on doctors examination.
Medical treatment with drugs such as Raloxifene, Tamoxifen and Anastrazole would help in reducing the estrogens (or theri effect) in the body. Surgery is also an option with a high success rate of complete cure (90%).
Mammography is the preferred method of detecting early Breast Cancer or to evaluate a breast lump. In fact it is the most reliable method of detecting a breast mass before it can even be felt by the examining hand. Slow growing tumours can be detected nearly 2 yrs before they can be felt by the doctor’s hand. Therefore routine screening is widely advised. On the brighter side only one third of the abnormalities detected by screening mammography are found to be cancerous. (Sensitivity 60-90%). The pick up rate depends on the patients age, breast density, tumour location and size, histology on biopsy. The tumour may be detected late in young women with dense breasts as compared to older women with fatty breasts.Smaller tumours especially those that aren’t calcified may also be more difficult to spot on the mammogram.
When should you get a routine mammogram done?
Different medical agencies have slightly different recommendations regarding the timing and the frequency of the screening tests. For the sake of not causing any confusion to the reader, let me tell you that screening mammogram can be started from the age of 40 yrs onwards. It must be done every year and must continue until that age of 74 yrs or till the estimated life expectancy is shorter than 7-10 years. The frequency can be reduced to once in 2 years after the age of 55 yrs. The doctors are advised to help the patient make informed decisions regarding the risk of false positives and over diagnosis Vs the benefits of early diagnosis.
What are the indications for mammography?
The following are some of the indications for mammography:
1. Routine screening in asymptomatic women
2. Evaluating after a diagnosis of Cancer is made and at regular intervals thereafter to monitor disease (same and opposite side)and response to treatment.
3. Evaluation of a breast mass (before biopsy)
4. Search of an occult breast cancer in those with a lymph node enlargement in the arm pit
5. Screening before cosmetic breast surgery.
Who has a high risk for breast cancer and would benefit from Routine mammography?
1. Age : risk of breast cancer rises rapidly until the early 60s, peaks at 70 and declines after that.
2. Positive Family history of Breast cancer or Ovarian Cancer. If a woman has a family history of 2 first degree relatives diagnosed <50 yrs of age especially if they are pre-menapausal, bilateral breast cancer or male breast cancer, that portends a higher risk.
3. Certain races – Ashkennazi jews and caucasian women are at a higher risk. People of Afro-caribbean descent have worse prognosis when they have breast cancer.
4. Hormonal exposure: Nulliparous women or those who have had their first pregnancy after the age of 30, early menarche (<12 yrs) and late natural menopause (>55yrs) are at a higher risk for breast cancer. Women on combined Oral contraceptive pills and those who receive post menopausal HRT with both Estrogens and Progesterones.
5. Life style: Obesity and lack of exercise, Alcohol intake and high dietary fat intake and a higher socioeconomic status can increase the risk too.
6. History of cancer: Women who have already had a cancer of one breast or of Endometrial cancer are at a higher risk for breast cancer.
7. Germline mutations in the BRCA family tumour suppressor genes (accounts for 5-10% of all cases -BRCA1 and BRCA 2), p53 gene mutations and those with Ataxia telangiectasia.
How do you interpret a mammogram?
1. To note down the indication for the test. Routine screening, accidentally detected breast lump (self detected or by the doctor), painful breast lump or other causes.
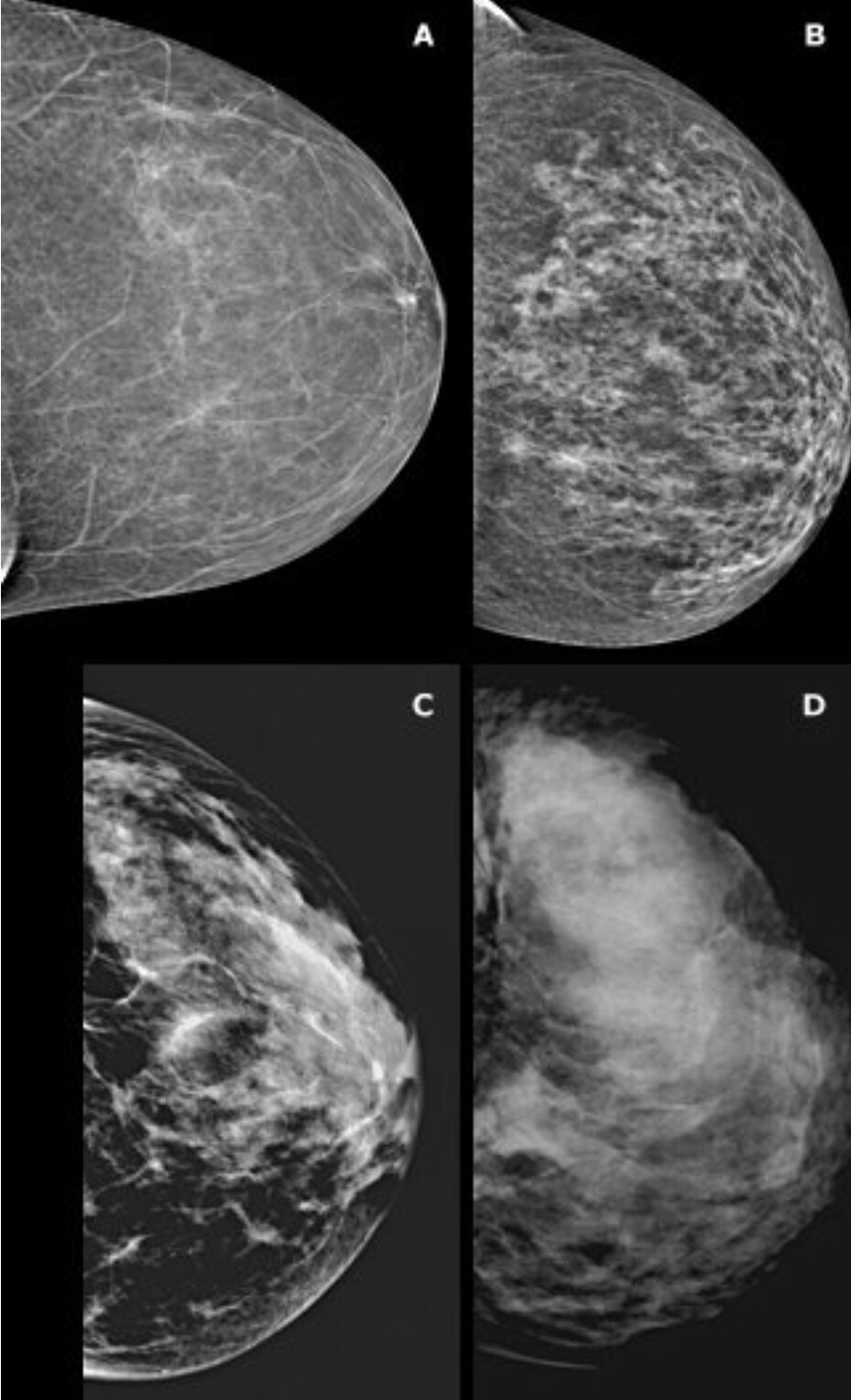
2. The Overall composition of the breast including its density. Younger women have denser breasts which reduce the sensitivity of the mammogram test in identifying sinister pathologies. The mammogram is more sensitive to pick up lesions in older women with fatty breasts (with less glandular breast tissue).
A – almost entirely fatty
B – Scattered areas of fibroglandular density
C – heterogeneously dense
D -extremely dense
3. Description of abnormalities: Density of breasts and calcific spots. Finely granular, popcorn like, vascular calcification suggest benign disease where as spiculated lesions, lesions with pleomorphic calcifications ( varies shapes and sizes), V or Y shaped calcifications would suggest an underlying neoplastic process.
4. The latest mammogram must be compared with the previously done study to look for interim changes and worsening of abnormalities.
5. The opinion must be summarised with advice for further management.
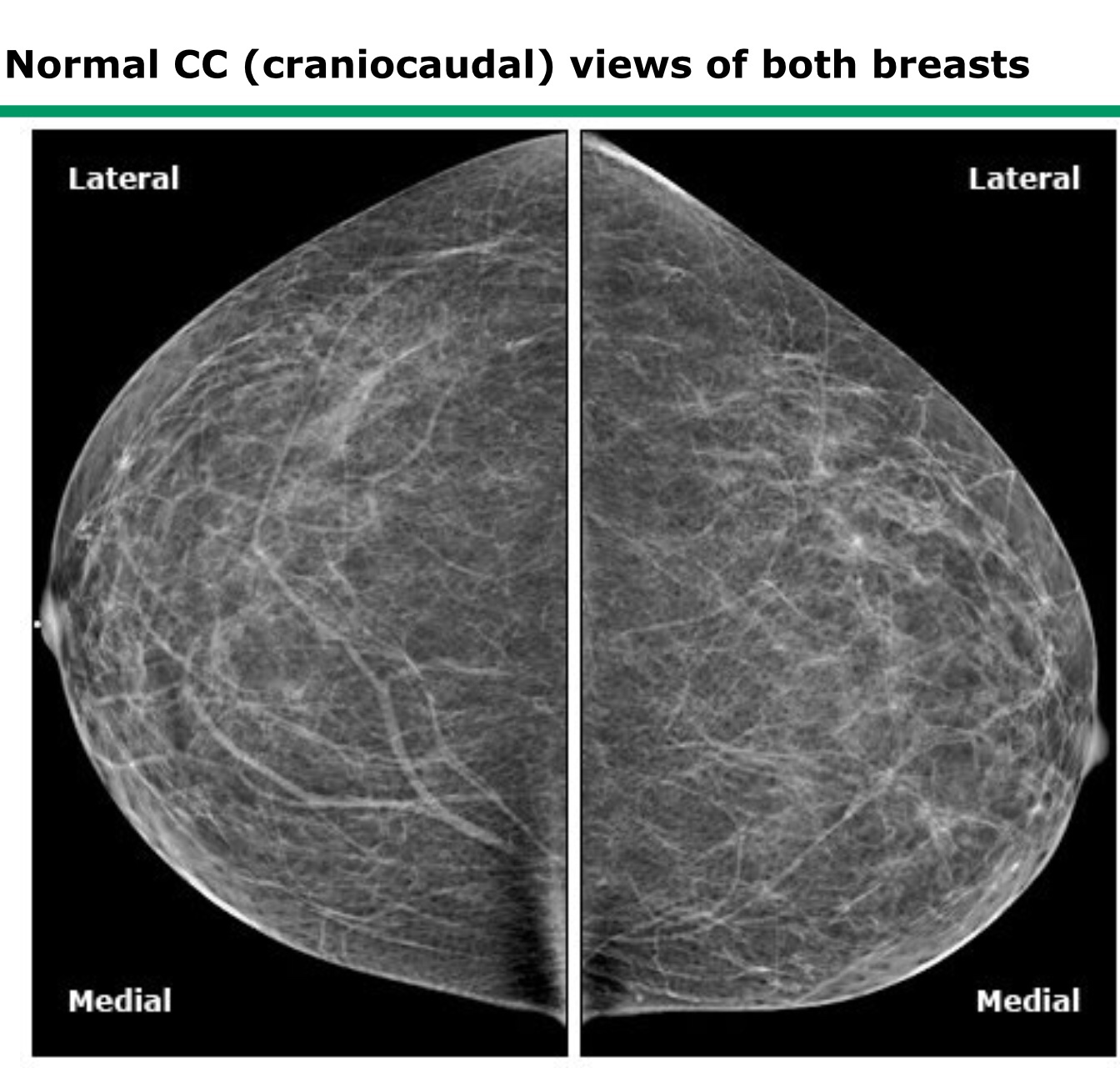
In a mammogram both breasts are viewed simultaneously as mirror images.The upper half in the craniocaudal view (CC) represents the outer portions of the breast and the lower half represents the inner parts of the breast.
H
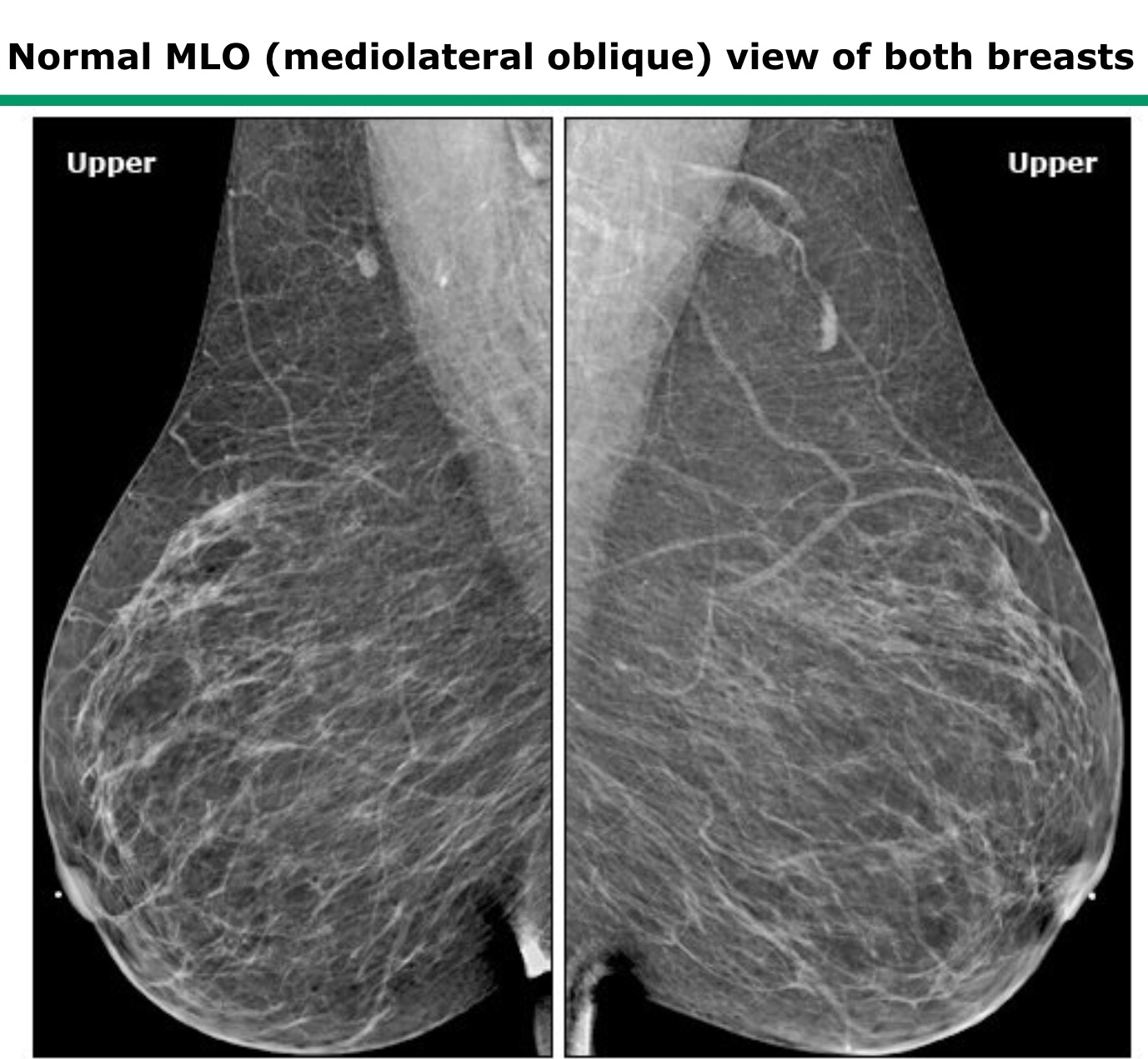
Correct positioning of the breasts would be very important in obtaining good pictures. In the MLO views the Pectoral muscle shadow must be seen and the breast must be adequately compressed to get the best pictures. Inadequate compression would cause superimposition of the tissues
Benign Breast lesions
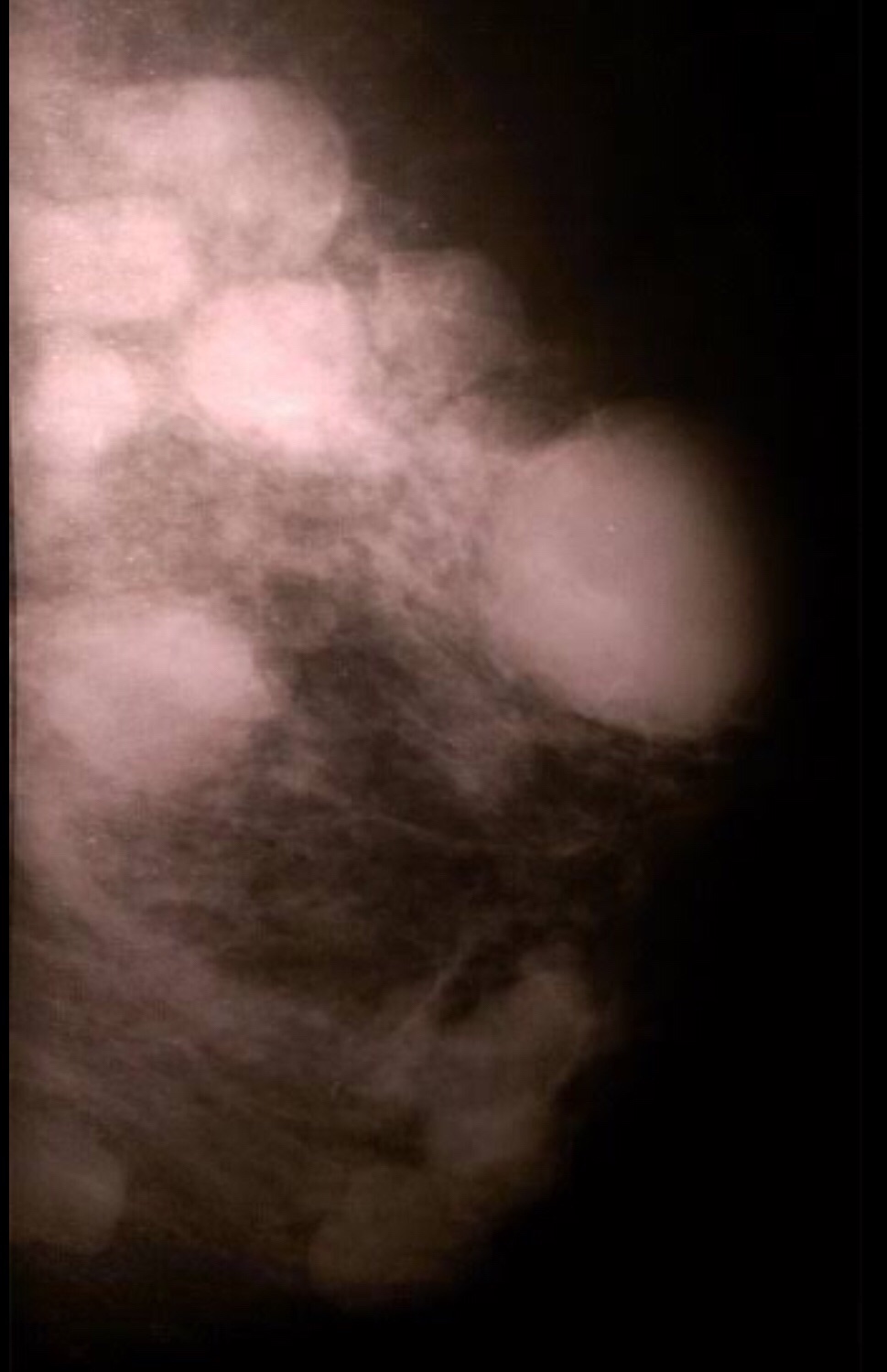
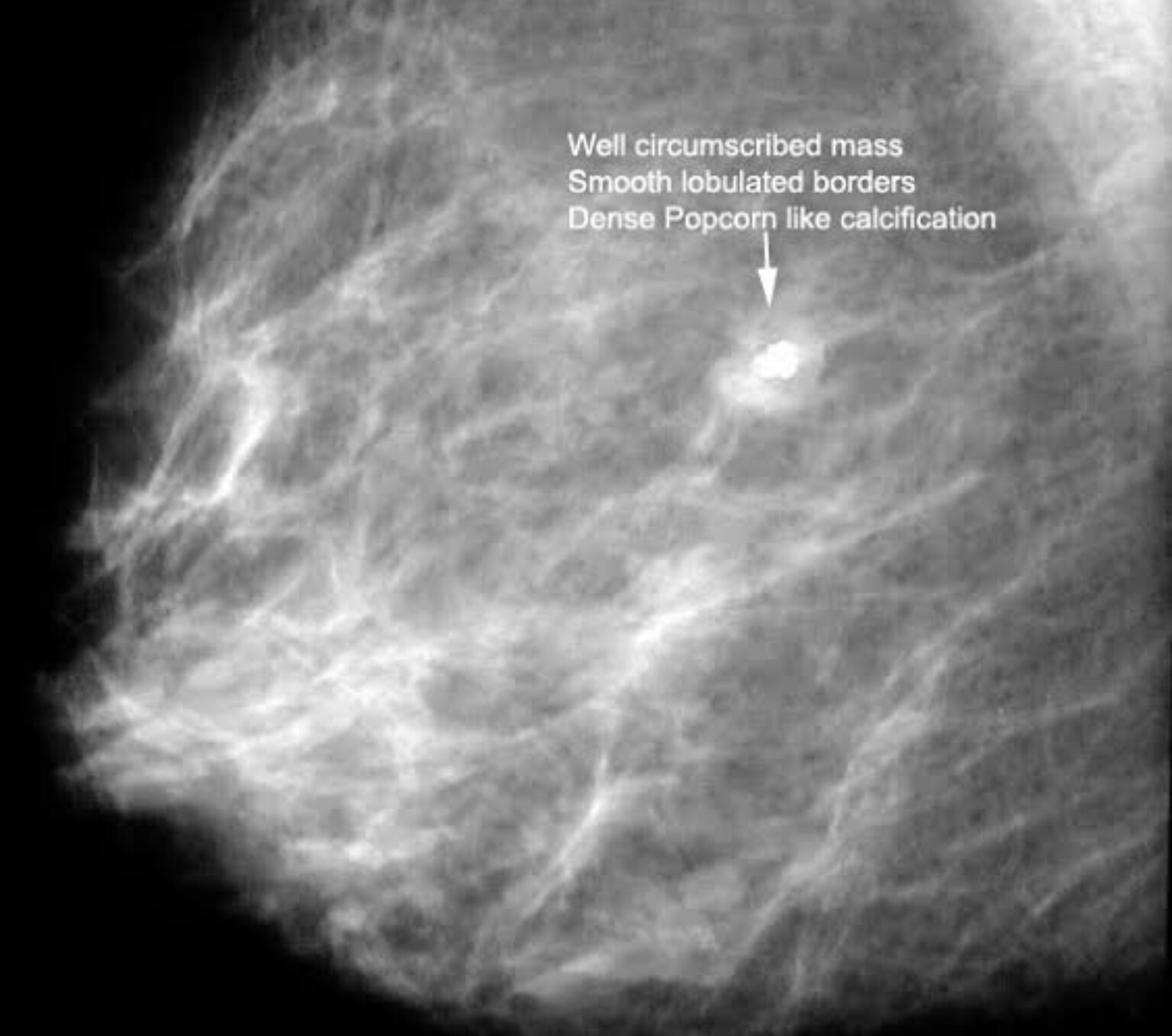
Fibroadenoma- is referred to as the Breast mouse- most often is detected as a small lump that moves inside the breast. They may be single or multiple as on the picture on the right below! The lumps are smooth walled and well defined.
The picture to the left shows a “popcorn” calcified Fibroadenoma.
Fibroadenosis: refer to lumpy breasts often painful with a rope like texture to feel. This condition is also referred to as Fibrocystic disease of the breast.
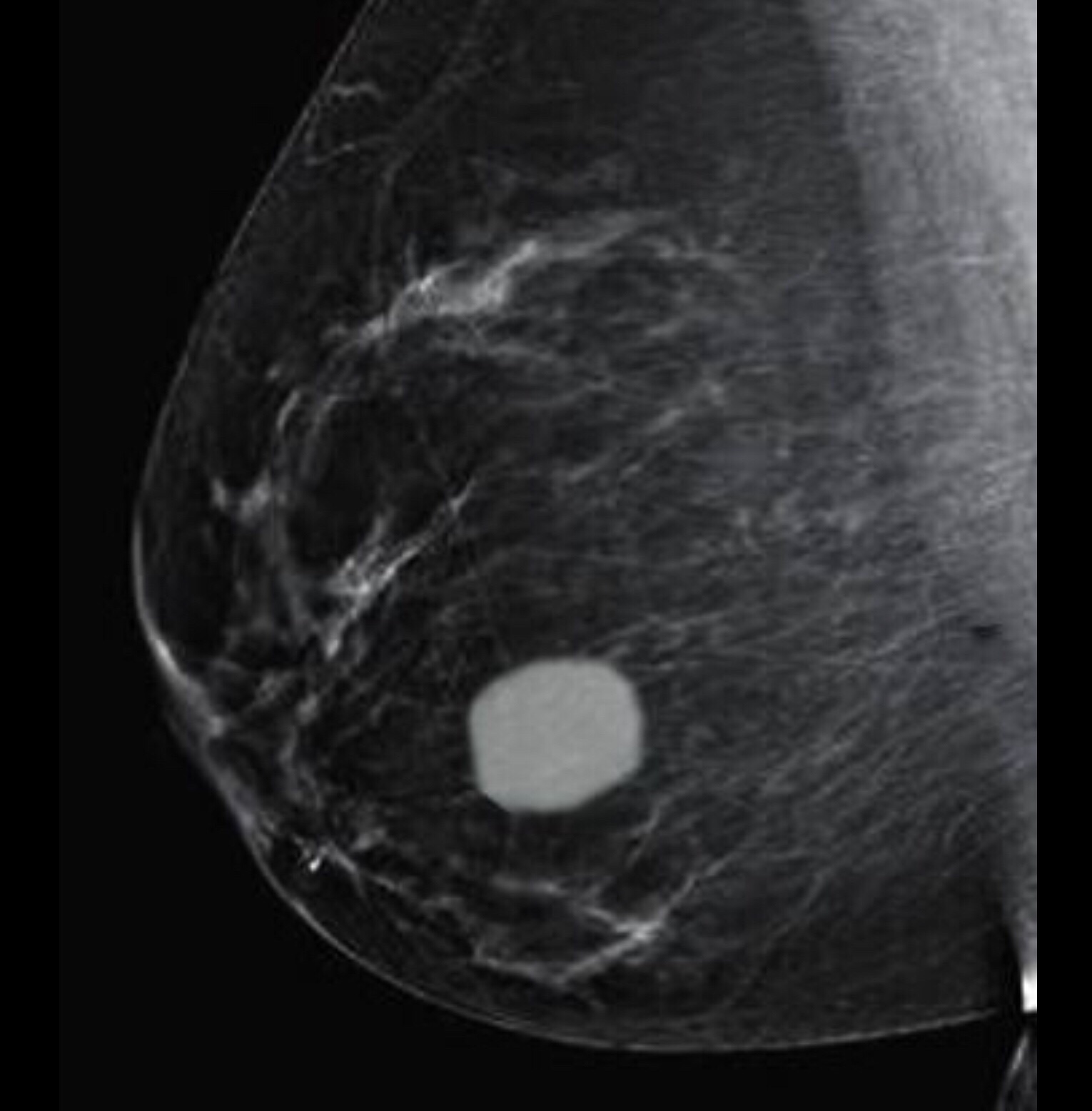
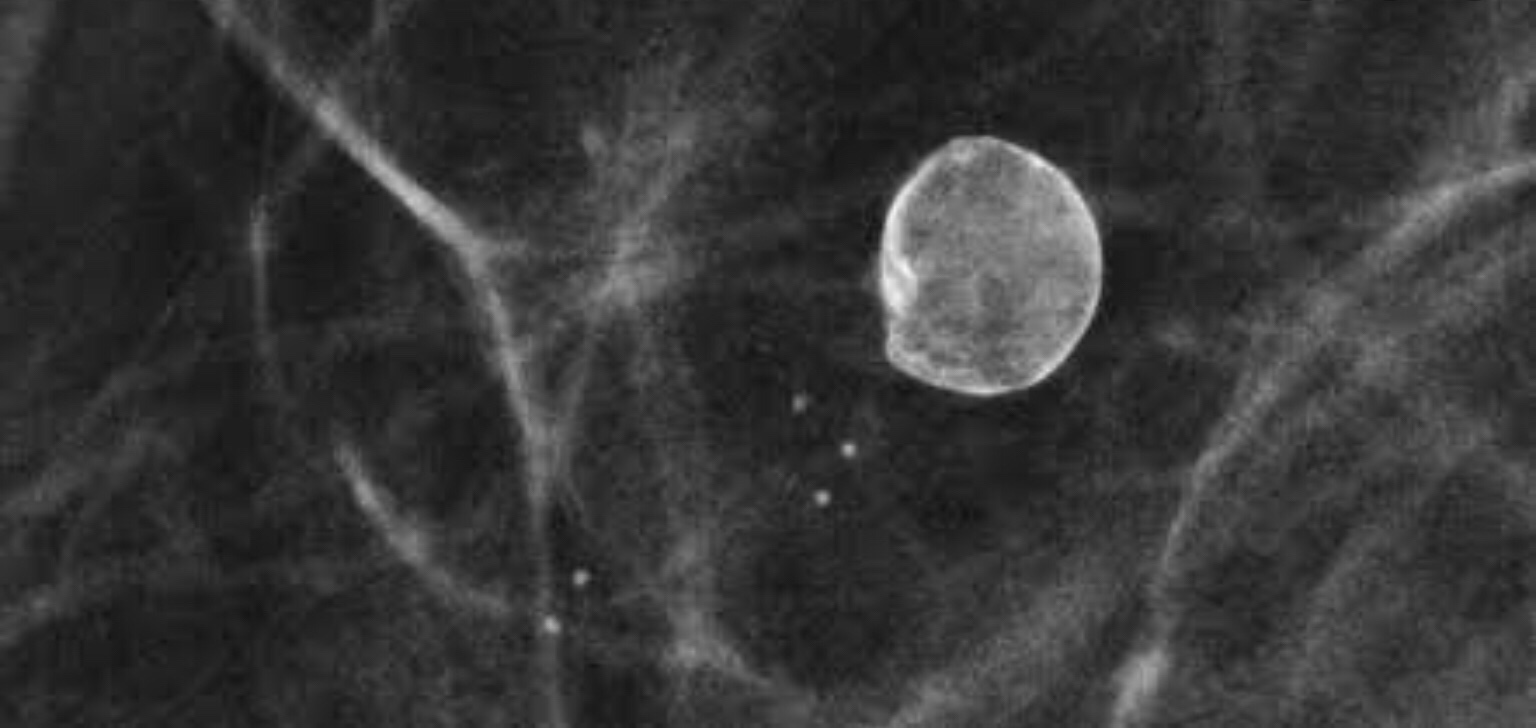
Simple Breast cyst: cysts are fluid containing cavities and are very well seen on the Ultrasound of the breast. But this is how they would appear on a mammogram. This thin walled cyst is accompanied by small smooth round to oval calcifications suggesting a benign lump.
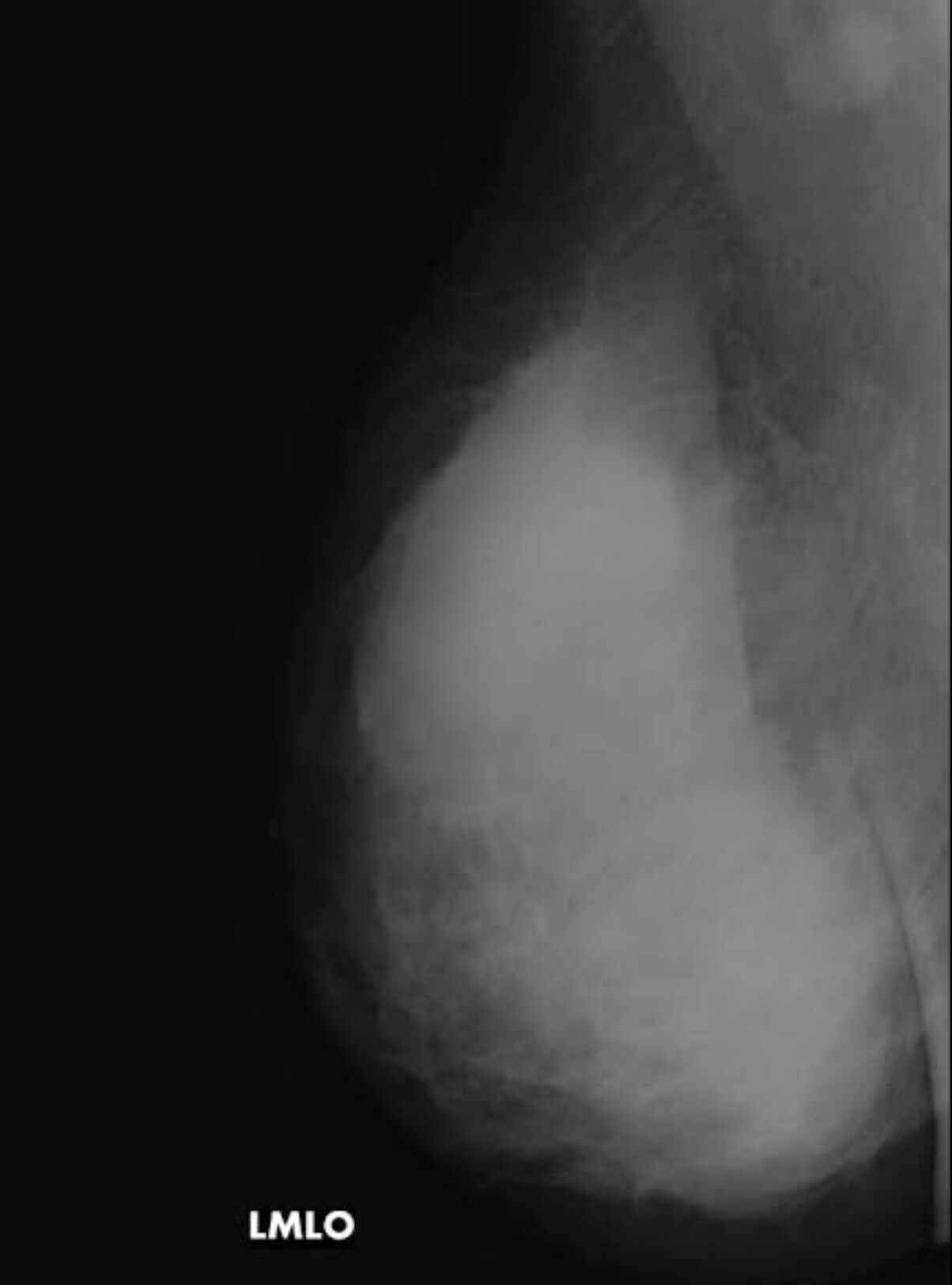
Breast Implants: Breast augmentation is one of the most common and popular cosmetic surgeries that women undergo. This is how they would appear on the mammogram.
Breast implants make mammography more difficult and can obscure small lesions. Mammography can also help detect implant related problems such as rupture, capsular contraction etc.
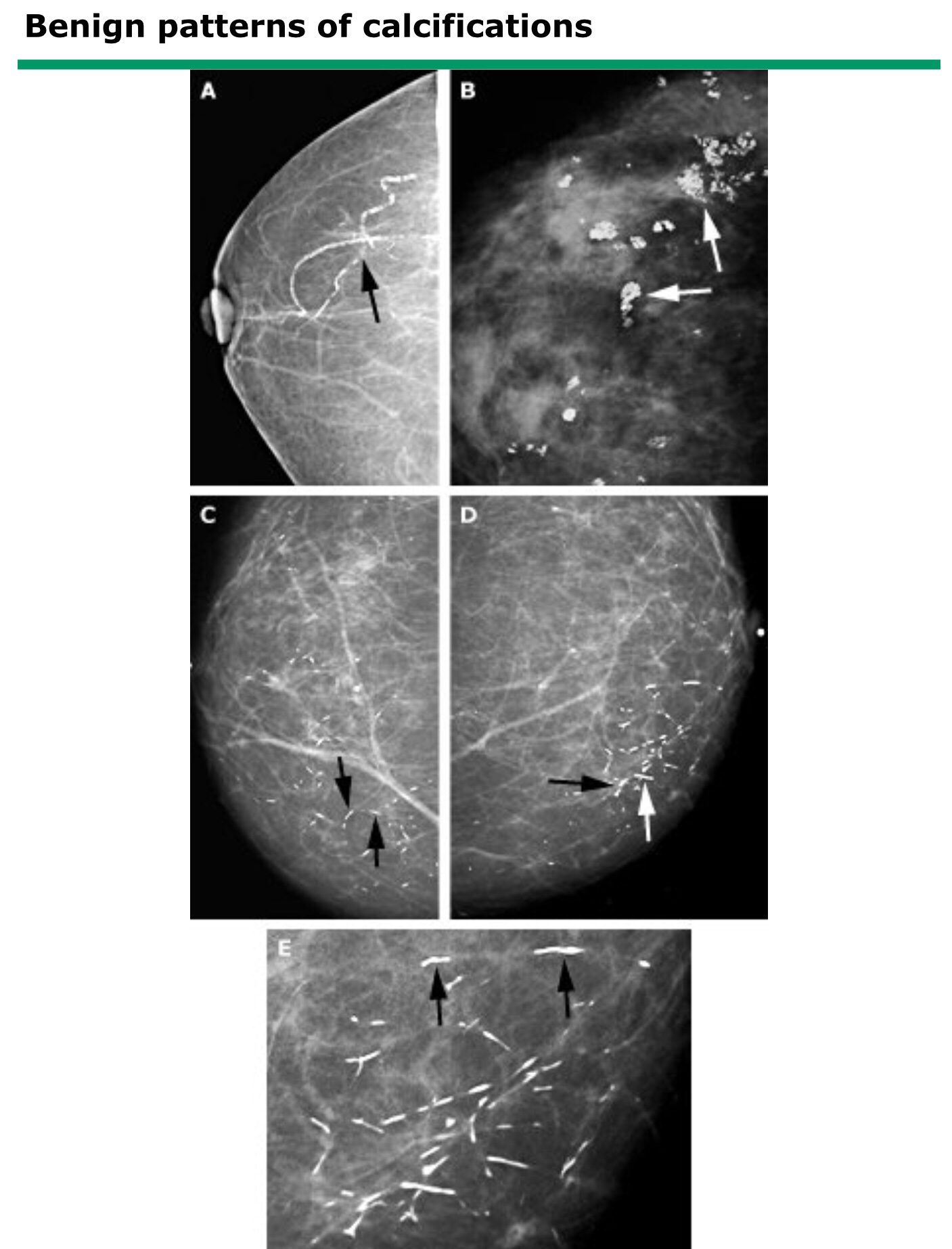
Benign Calcification of the breast:
A – vascular calcifications
B – popcorn calcification
C & D – benign secretory calcifications
E – cigar shaped calcifications.
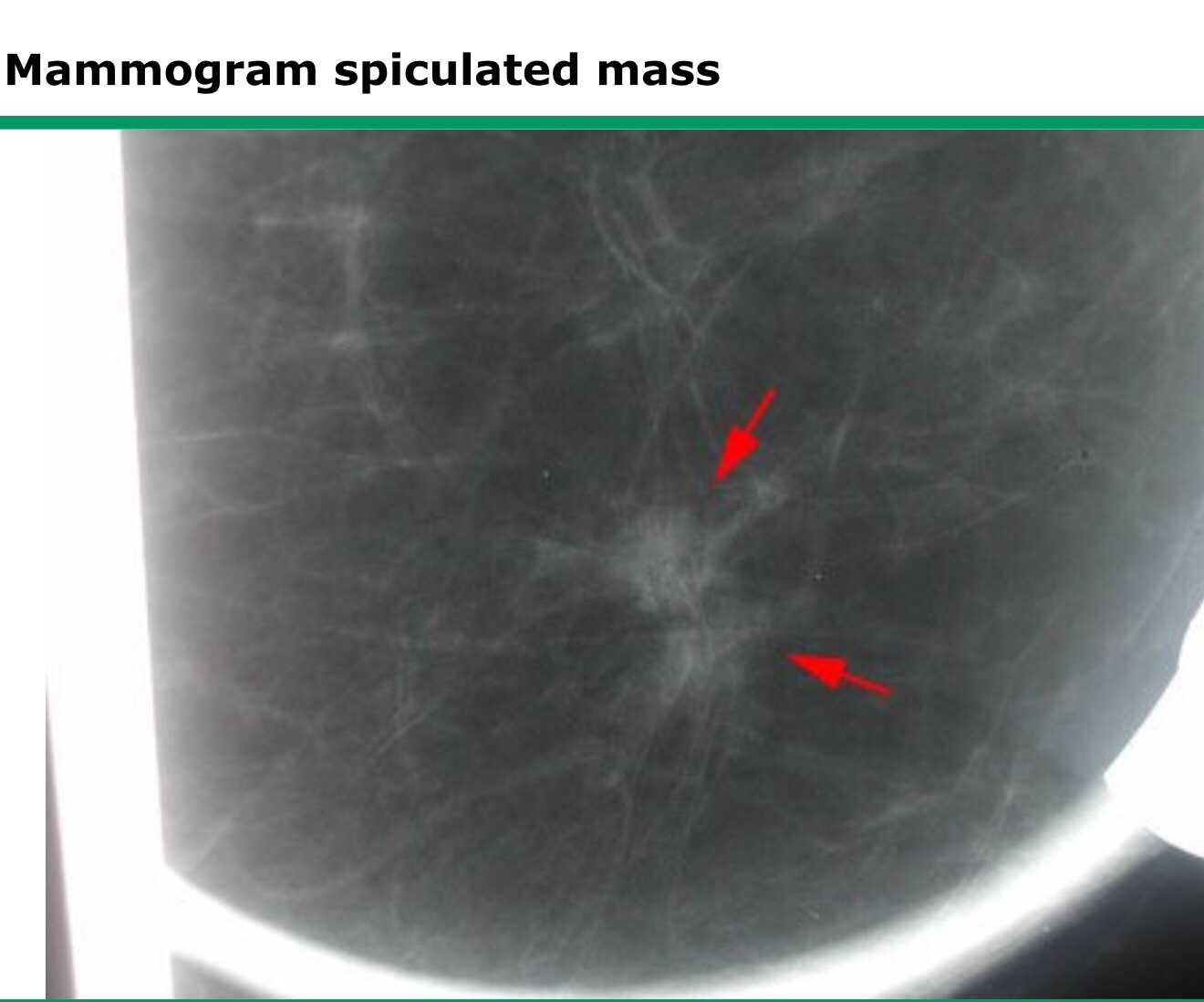
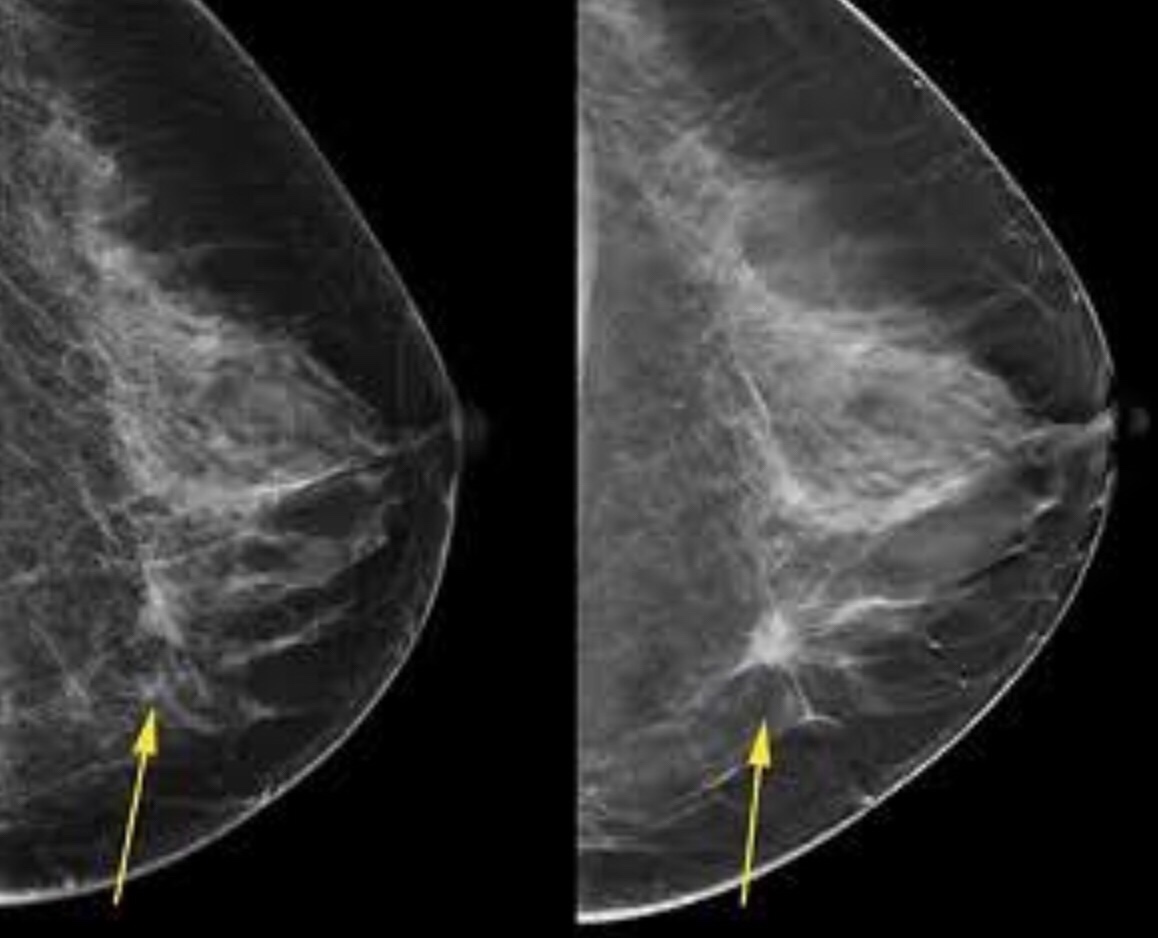
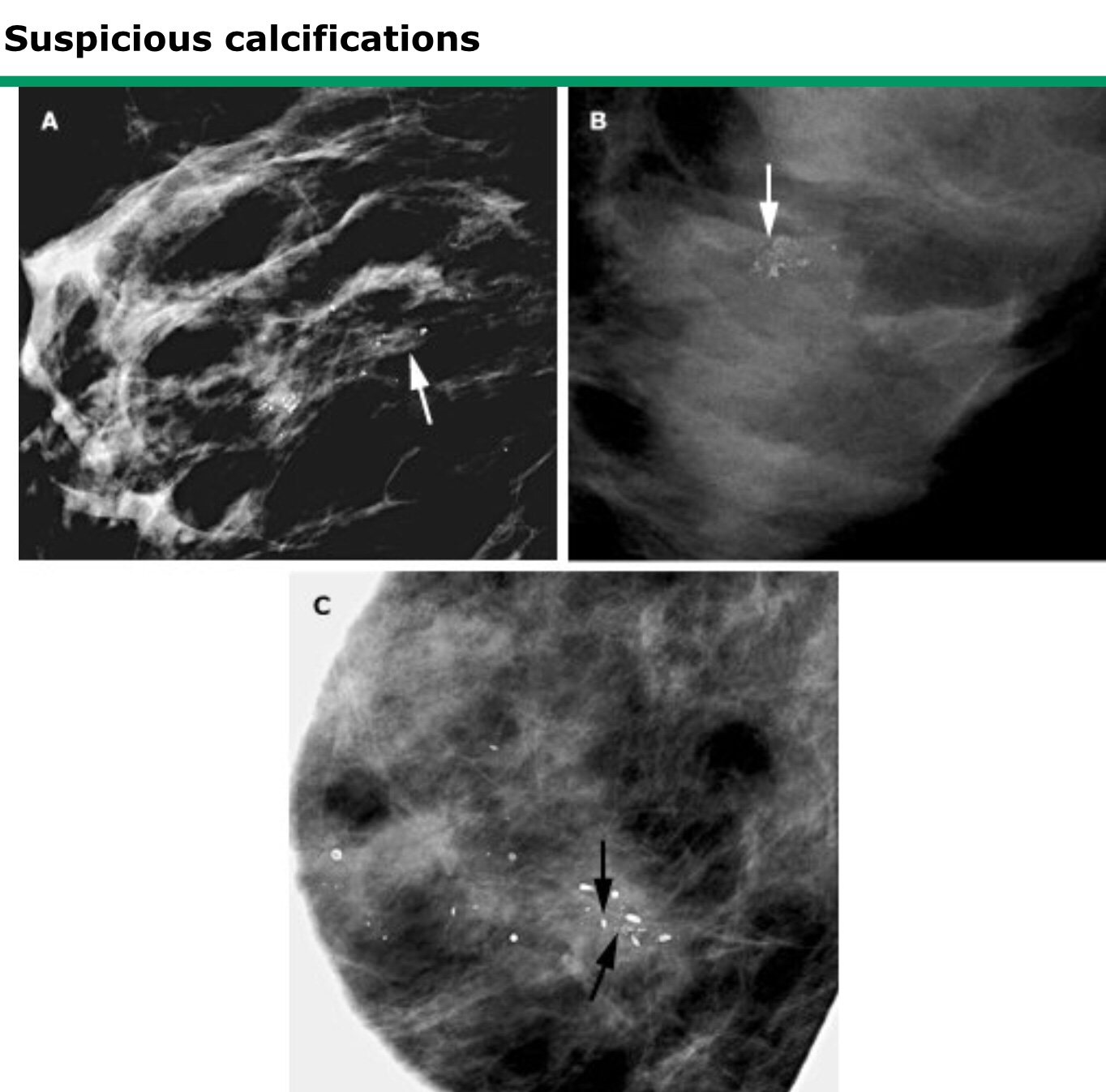
Malignant lesions:
Spiculated lesions with greater density indicate malignancy. Certain patterns of calcification also suggest malignancy.
Clustered irregular microcacifications also suggest malignancy especially when there is distortion of the surrounding breast tissue. V and Y shaped calcifications also suggest malignancy.
What should you do after getting the mammogram report?
The first thing that you should do with the mammogram is to show it to your doctor and ask him for his interpretation and advice. He might suggest that nothing needs to be done or he may ask you to repeat the test after a few months or he may ask for a few additional test such as an Ultrasound scan or an MRI of the breast. He may even advice you regarding a needle biopsy or surgery.
To summarise
Mammography is more sensitive in picking up lesions in the breast compared to examination by a doctor.
Birads 0,4 &5 require further evaluation. Birads 1 is a normal study. Birads would mean a benign disease of the breast. Birad 3 would mean that the test would need to be repeated after 6 months. A report of Birads 4 and 5 will be followed by a biopsy.
An MRI may be done for women with a high risk for breast cancer in addition to a Digital Mammogram (women with BRCA mutations, history of childhood radiation to the chest, a higher lifetime risk for breast cancer 20% and previous history of breast cancer) An MRI breast would also be useful in women with breast implants especially to detect rupture of implant.
An USG of the breast might be useful to differentiate solid from cystic (fluid filled) lumps of the breast.



You must be logged in to post a comment.